 Ευαγγελάτος Γεώργιος")
COVID-19 is not “just another flu”: a real-life comparison of severe COVID-19 and influenza in hospitalized patients in Vienna, Austria
Team members
Infection (2021)
Abstract
Background
COVID-19 is regularly compared to influenza. Mortality and case-fatality rates vary widely depending on incidence of COVID-19 and the testing policy in affected countries. To date, data comparing hospitalized patients with COVID-19 and influenza is scarce.
Methods
Data from patients with COVID-19 were compared to patients infected with influenza A (InfA) and B (InfB) virus during the 2017/18 and 2018/19 seasons. All patients were ≥ 18 years old, had PCR-confirmed infection and needed hospital treatment. Demographic data, medical history, length-of-stay (LOS), complications including in-hospital mortality were analyzed.
Results
In total, 142 patients with COVID-19 were compared to 266 patients with InfA and 300 with InfB. Differences in median age (COVID-19 70.5 years vs InfA 70 years and InfB 77 years, p < 0.001) and laboratory results were observed. COVID-19 patients had fewer comorbidities, but complications (respiratory insufficiency, pneumonia, acute kidney injury, acute heart failure and death) occurred more frequently.
Median length-of-stay (LOS) was longer in COVID-19 patients (12 days vs InfA 7 days vs. InfB 7 days, p < 0.001). There was a fourfold higher in-hospital mortality in COVID-19 patients (23.2%) when compared with InfA (5.6%) or InfB (4.7%; p < 0.001).
Conclusion
In hospitalized patients, COVID-19 is associated with longer LOS, a higher number of complications and higher in-hospital mortality compared to influenza, even in a population with fewer co-morbidities. This data, a high reproduction number and limited treatment options, alongside excess mortality during the SARS-CoV-2 pandemic, support the containment strategies implemented by most authorities.
Introduction
As of July 26th 2020, the ongoing SARS-CoV-2 pandemic has infected over 68 million people and has caused over 1,560,000 deaths worldwide [1], challenging affected countries and healthcare systems. The pandemic has impacted the lives of billions on multiple levels and has had a major impact on the world economy [2].
Influenza viruses are highly contagious and during seasonal epidemics excess mortality is observed. While therapeutic options and vaccinations exist for influenza vaccination rollout for COVID-19 is still limited and delayed by supply problems, and whilst there is growing evidence that certain drugs may be effective, these are still deemed to have limited therapeutic effect [3,4,5,6,7,8,9,10]. In comparison to COVID-19 there are no strict regulations and containment strategies during seasonal influenza virus epidemics.
While mortality and case-fatality-rates of COVID-19 seem to be higher than for influenza A (InfA) and influenza B (InfB), reliable information is difficult to obtain due to asymptomatic and oligosymptomatic presentations in both cases. Asymptomatic cases are described in 18–75% for SARS-CoV-2 [11, 12]) and 4–85% for influenza [13]. Case-fatality rate estimates range from 0.25 to 5.7% for COVID-19 [14, 15] and from 0.1 to 1% for influenza [16].
Here we compare the demographic data, medical history, length-of-stay (LOS), complications including ICU admission and in-hospital mortality between hospitalized PCR confirmed patients with COVID-19, InfA and InfB. Treatment and isolation were performed at the same department by the same specialists for infectious diseases, ensuring equal quality of medical care.
Methods
Study design and data gathering
This study was conducted at the Department for Infectious Diseases and Tropical Medicine at the Kaiser-Franz-Josef Hospital in Vienna, Austria. We compared demographics, medical history, laboratory results, LOS and complications including ICU admission and in-hospital mortality of patients with polymerase chain reaction (PCR)-proven COVID-19, InfA and InfB virus infections.
Data from COVID-19 patients were collected from March 1st to April 25th 2020. PCR testing for SARS-CoV-2 took place at our hospital’s laboratory institute or at other certified laboratories in Vienna. Data from all subsequent influenza patients were collected retrospectively in 2017/18 and prospectively in 2018/19. Influenza diagnosis was made at the emergency department before admission using the Alere™ i Influenza A & B assay (Alere, Waltham, MA, USA) in 2017/18 and the Cobas® Liat® point-of-care test (POCT) from Roche (Roche Molecular Systems, Pleasanton, CA, USA) in 2018/19.
All hospitalized patients ≥ 18 years with molecular proven COVID-19 or influenza were eligible for the study. Patients’ medical history, laboratory parameters and complications were collected via a standardized form during hospital admission. Incomplete data were updated retrospectively from patients’ electronic health records whenever possible.
The study was approved by the local ethics committee.
Definition of variables
The first day of any COVID-19 or influenza-associated symptom was considered to be disease onset. Fever was defined as a body temperature ≥ 38 °C. Dehydration was defined as the need for intravenous fluids based on clinical appearance. Respiratory insufficiency was defined as SpO2 ≤ 93% at room air or the need for supplementary oxygen based on clinical judgment by the treating physician. Pneumonia was defined as typical consolidation and/or opacity on a radiological image. Myositis was defined as a creatine-kinase (CK) level above 1000 U/L. Heart failure was defined by new onset or worsening of peripheral edema and/or congestion on X-ray in patients with history of chronic heart failure and without any other cause. Acute kidney injury was defined as either an increase of creatinine level by 0.3 mg/dl from the baseline kidney function within 48 h or an increase of ≥ 1.5 times the baseline (presumed to have occurred within the previous 7 days due to the current episode of illness). When no previous creatinine level was available as baseline, the acute kidney injury was assessed retrospectively. We did not differentiate between complications which were present on admission or developed during admission.
Statistical analysis
Data were double-checked, entered in a MS Excel sheet (Microsoft, Redmond, WA, USA) and anonymized before statistical analysis. The statistical analyses were performed with SAS V9.4 and R Version4.0.2. Categorical variables were described by counts and percentages. For metric non-normally distributed variables the median (Md) and interquartile range (IQR) were used. Significance tests for categorical variables were made via cross tables and Chi-squared test or Fisher’s exact test, where applicable. Kruskal–Wallis tests were performed to compare the three groups (InfA, InfB and COVID-19) for metric non-normally distributed variables. A two-sided alpha < 0.05 was considered statistically significant.
To check for difference in binary outcomes (e.g. acute heart failure, in-hospital mortality) logistic regression analyses were performed with the factor group (InfA, InfB vs COVID-19). Odds ratios and two-sided 95% confidence intervals reported.
For in-hospital mortality and discharged alive from hospital analysis, competing risk analysis was performed and the cumulative incidence curves were compared using Gray’s test (Gray 1988).
Results
Patients demographics and medical history
The total population consisted of 708 patients, 142 (20.1%) had COVID-19, 266 (37.6%) InfA and 300 (42.3%) InfB. 356 (50.3%) were male, with a higher proportion of male patients in the COVID-19 group. Overall median age was 73.5 years (61–82) and varied between groups (p < 0.001); overall InfB patients were oldest.
Differences in medical history were demonstrated between the groups, with lower rates of chronic kidney disease (p < 0.001) and chronic obstructive disease (p = 0.002) in the COVID-19 group. Median time from symptom onset to hospitalization was 7 days (IQR 3–10) in the COVID-19 group and differed significantly from InfA (2 days; IQR 1–4) and InfB (2 days; IQR 0.8–4) positive patients (p < 0.001). Antiviral treatment differed significantly between groups (p < 0.001), while antibiotic prescription rates did not yield a statistical significance (p = 0.11). For details see Table 1.
Table 1 Patients demographics and medical history
| Total (n = 708) |
SARS-CoV-2 (n = 142) |
Influenza A (n = 266) |
Influenza B (n = 300) |
p value | |
|---|---|---|---|---|---|
| Age (years)a | 73.5 (61–82) | 70.5 (53–80) | 70 (58–80) | 77 (67–85) | < 0.001 |
| Sex (male) | 356/708 (50.3%) | 84 (59.2%) | 131 (49.3%) | 141 (47%) | 0.053 |
| BMI (kg/m2) | 25.6 (22.7–30.1) [n = 488]b | 25.9 (24.2) [n = 75] | 25.3 (22.2–29.7) [n = 218] | 26 (23–30.5) [n = 195] | 0.246 |
| Time from symptom onset to hospitalization | 3 days (1–5) n = 616 | 7 days (3–10) n = 126 | 2 days (1–4) n = 244 | 2 days (0.8–4) n = 246 | < 0.001 |
| Antiviral treatment | 433 (61.1%) | 67 (47.2%)c | 188 (70.7%)d | 178 (59.3%)d | < 0.001 |
| Antibiotic treatment | 282 (39.8%) | 46 (32.4%) | 114 (42.9%) | 122 (40.7%) | 0.112 |
| Medical history | |||||
| Chronic kidney disease | 212 (29.9%) | 26 (18 .3%) | 75 (28.2%) | 111 (37%) | < 0.001 |
| Obstructive pulmonary disease | 194 (27.4%) | 23 (16.2%) | 92 (34.6%) | 79 (26.3%) | < 0.001 |
| Diabetes | 176 (24.9) | 27 (19%) | 69 (25.9%) | 80 (26.7%) | 0.193 |
| Atrial fibrillation | 133 (18.8%) | 30 (21.1%) | 46 (17.3%) | 57 (19%) | 0.635 |
| Coronary heart disease | 48/312 (15.4%) | 20/142(14.1%) | 28/170 (16.5%) | NA | 0.56 |
| Any malignancy | 94 (13.3%) | 12 (8.5%) | 31 (11.7%) | 51 (17%) | 0.029 |
| Dementia | 82 (11.6%) | 12 (8.5%) | 30 (11.3%) | 40 (13.3%) | 0.142 |
| Congestive heart failure | 75 (10.6%) | 17 (12%) | 28 (10.5%) | 30 (10%) | 0.82 |
| Peripheral artery disease | 45/707 (6.4%) | 7/141 (5%) | 14 (5.3%) | 24 (8%) | 0.309 |
| Rheumatic disease | 11/312 (3.5%) | 6 (4.2%) | 5/170 (2.9%) | NA | 0.54 |
- Significant differences are marked in bold
- NA not available (data were not available in this subgroup)
- aMedian and interquartile range are shown
- bIf data were not available for all patients, the number of valid observations per variable and group is additionally reported with n = for numeric data as ratio x/n for binary data in the respective cell
- c44 patients received lopinavir/ritonavir, 18 hydroxychloroquine, one both drugs, one lopinavir/ritonavir plus remdesivir, three camostat; oseltamivir
- dOseltamivir was used as antiviral treatment
Laboratory parameters on admission
All laboratory parameters except creatine-kinase (p = 0.115) and bilirubin (p = 0.062) differed significantly between groups. COVID-19 patients had the lowest leukocyte count (p < 0.001), highest C-reactive-protein (p < 0.001) and lactate-dehydrogenase level (p < 0.001). For further details see Table 2.
Table 2 Laboratory parameters on admission
Name (unit) [n] Total
(n = 708)SARS-CoV-2
(n = 142)Influenza A
(n = 266)Influenza B
(n = 300)p value Leukocytes (G/L) 6.8 (5–9.2) n = 704 5.9 (4.5–7.4) n = 139 7.7 (5.8–10.1) n = 265 6.8 (5–9.2) < 0.001 Platelets (G/L) 194 (149–249) n = 704 200 (155–255) n = 139 199 (158–256) n = 265 185 (143–238) 0.030 C-reactive protein (mg/L) 34.3 (14.9–72.8) n = 702 60 (27.9–95.7) n = 137 40 (21–77) n = 265 23 (10–54) < 0.001 Creatinine (mg/dl) 1.00 (0.8–1.3) n = 700 1 (0.8–1.3) n = 138 0.93 (0.73–1.19) n = 263 1.04 (0.85–1.39) n = 299 < 0.001 CK (U/L) 117 (65–223) n = 630 104 (52–202) n = 124 119 (62–246) n = 242 119 (73–214) n = 264 0.115 ALT (U/L) 28 (18–40) n = 339 31 (19–43) n = 125 25 (17–34) n = 174 38 (24–57) n = 40 < 0.001 Bilirubin (mg/dl) 0.5 (0.3–0.7) n = 643 0.5 (0.35–0.69) n = 131 0.45 (0.28–0.63) n = 242 0.45 (0.31–0.66) n = 270 0.062 LDH (U/L) 245 (205–312) n = 453 303 (234–382) n = 121 229 (194–282) n = 165 233 (203–289) n = 165 < 0.001 Troponin T-hs (ng/L) 18 (8.3–43.2) n = 174 13 (7–28) n = 94 22 (13–47) n = 45 26 (9–69) n = 35 0.005 - Not every information was available for each patient on admission, in such cases the number of valid observations per variable and group is reported with n = in the respective cell
- Significant differences are marked in bold
- IQR interquartile range, CK creatinine-kinase, ALAT alanine-amino-transferase, GGT gamma-glutamyl-transferase, AP alkalic phosphatase, LDH lactate-dehydrogenase, eGFR estimated glomerular-filtration-rate ap-values derive from Kruskal–Wallis test
Complications and outcome
COVID-19 infected patients had a significantly higher rate of respiratory insufficiency (COVID-19 66.9% vs 36.8% InfA vs 18.3% InfB, p < 0.001), pneumonia (COVID-19 76.1% vs 26.3% InfA vs 24% InfB, p < 0.001), acute kidney injury (COVID-19 27.5% vs 10.9% InfA vs 13.8% InfB, p < 0.001) and acute heart failure (COVID-19 10.6% vs 4.1% InfA vs 3.7% InfB, p = 0.006). The myositis rate was higher in influenza patients (InfA: 7.7%, InfB 8.1%) compared to COVID-19 (3.5%), but this was not statistically significant (p = 0.19) and the rate of acute coronary syndrome did not differ between groups. Odds ratios and 95% confidence intervals are presented in Fig. 1.
Fig. 1
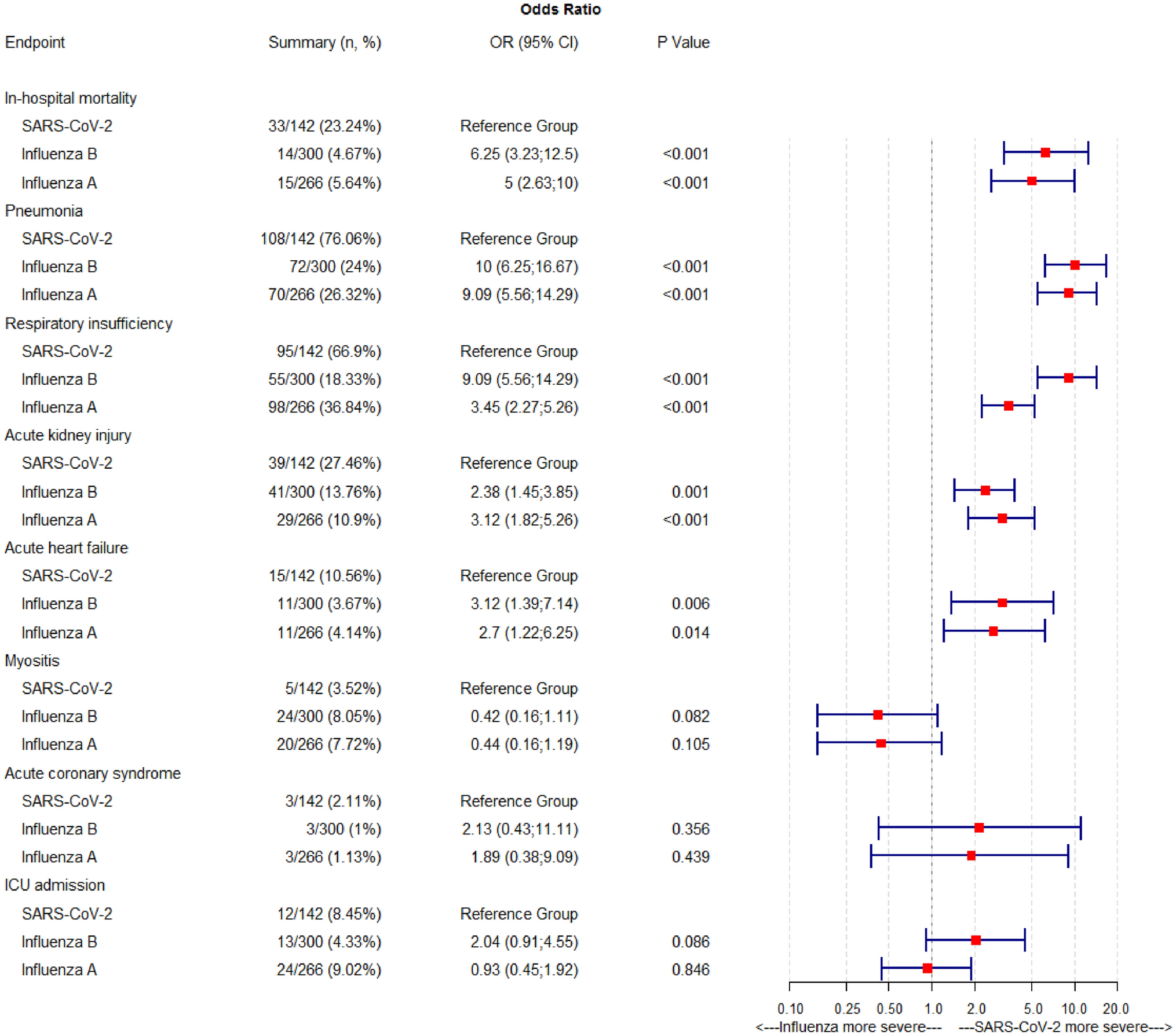
Complications and outcome. Data are expressed as inverse OR. OR > 1, therefore, means the risk for the complication is higher in the SARS-CoV-2 group (e.g.: an OR of 6.25 in the InfB line for in-hospital mortality means the risk for in-hospital mortality is 6.25 times higher for COVID-19 patients. ICU intensive care unit
In-hospital mortality differed significantly between groups with 23.2% for COVID-19, 5.6% for InfA and 4.7% for InfB (p < 0.001). COVID-19 had a higher in-hospital mortality compared to InfA (OR 5; 95% CI 2.63–10) and InfB (OR 6.25; 95% CI 3.23–12.5), see Fig. 1. The cumulative incidence curves for in-hospital mortality and discharge from hospital also yielded statistically significant differences (see Fig. 2). The median time to patients being discharged from hospital (length of stay, LOS) is almost double for COVID-19 patients when compared to those with InfA and InfB (12 days vs 7 days, respectively). The groups did not reach statistically significant differences with respect to ICU admission rates (COVID-19 8.5% vs InfA 9% vs InfB 4.3%, p = 0.065). For further details see Fig. 1.
-
Fig. 2
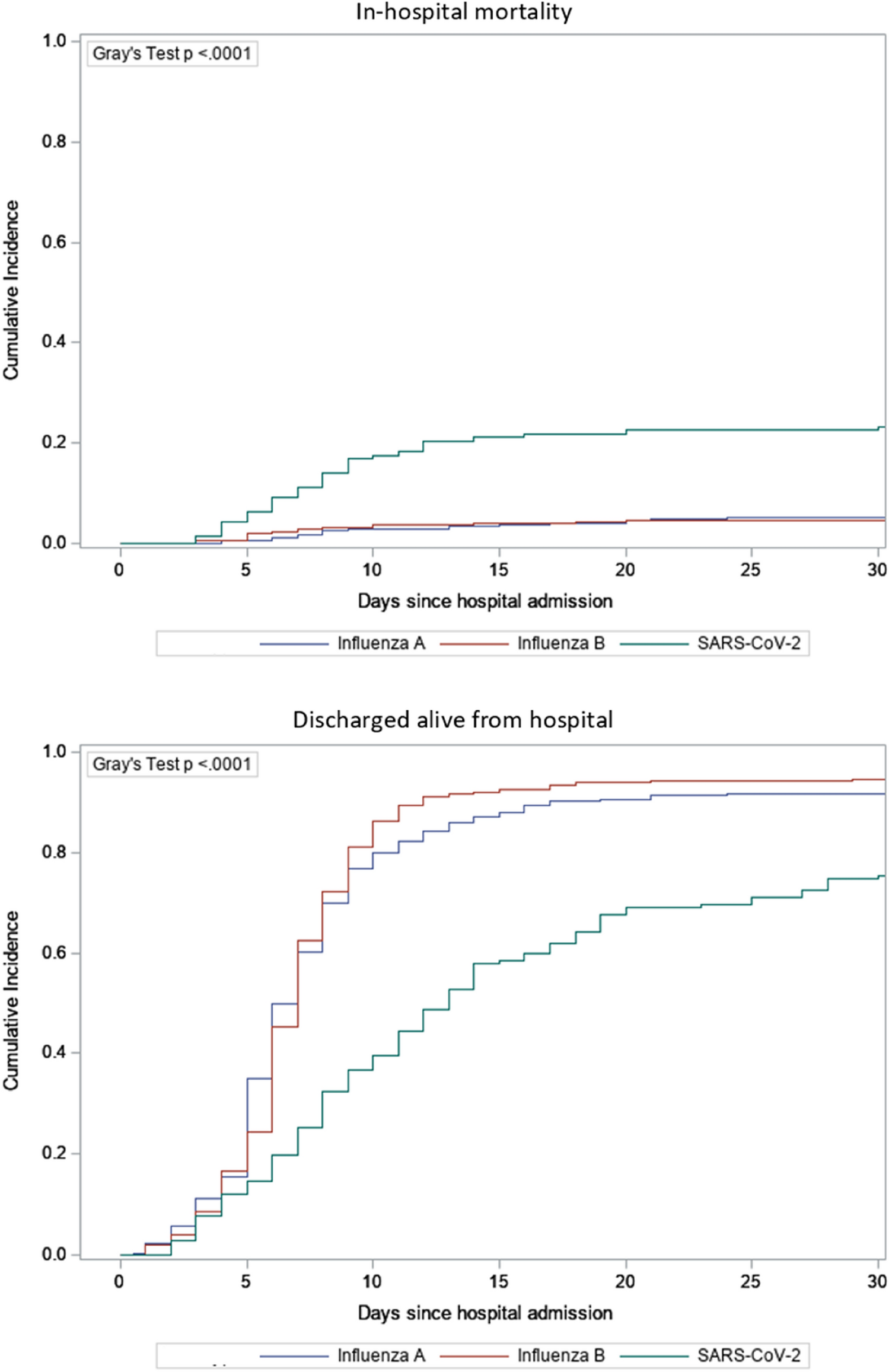
Cumulative incidence curves for in-hospital mortality and discharged-alive from hospital
Mortality was strongly associated with older age in all groups. No patient under 60 died due to COVID-19 or influenza. Difference in in-hospital mortality increased with older age and was 2–13 times higher for COVID-19 compared to InfA or InfB when analyzing the age groups 61–70 years, 71–80 years, 81–90 years and > 90 years. For details see Table 3 and Fig. 3.
Table 3 Age group-specific in-hospital mortality rate and ICU admission rate
< 60 years 61–70 years 71–80 years 81–90 years > 90 years Total In-hospital mortality SARS-CoV-2 0/47 (0%) 2/23 (8.7%) 8/38 (21.1%) 18/28 (64.3%) 5/6 (83.3%) 33/142 (23.2%) Influenza A 0/77 (0%) 3/61 (4.9%) 2/62 (3.2%) 7/55 (12.7%) 3/11 (27.3%) 15/266 (5.6%) Influenza B 0/48 (0%) 2/50 (4%) 3/94 (3.2%) 5/84 (6%) 4/24 (16.7%) 14/300 (4.7%) ICU admission rate SARS-CoV-2 5/42 (10.6%) 3/23 (13%) 4/38 (10.5%) 0/28 (0%) 0/6 (0%) 12/142 (8.5%) Influenza A 9/77 (11.7%) 8/61 (13.1%) 4/62 (6.5%) 3/55 (5.5%) 0/11 (0%) 24/266 (9%) Influenza B 5/48 (10%) 1/50 (2%) 4/94 (4.3%) 3/84 (3.6%) 0/24 (0%) 14/300 (4.3%) Fig. 3 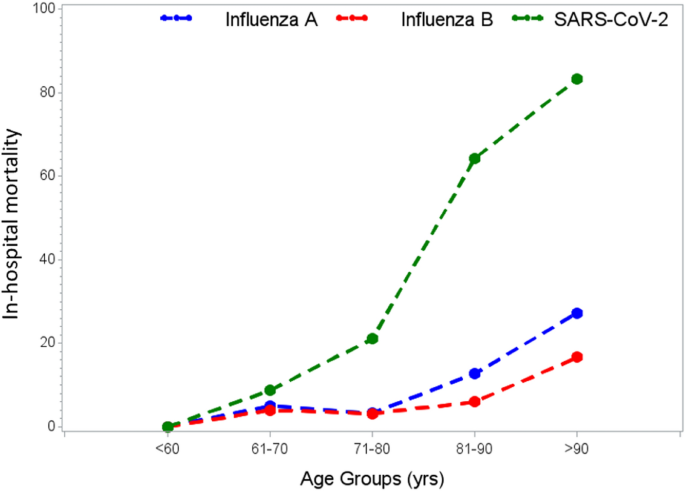
Age group-specific in-hospital mortality rate
Age group specific ICU admission rates are shown in Table 3. About 10% of patients under 60 years were admitted to the ICU. The rate decreased with higher age.
Antimicrobial therapy
The use of antiviral treatment did differ significantly between COVID-19, influenza A and influenza B (COVID-19 47.2%, InfA 70.7%, InfB 59.3%, p ≤ 0.001). While antiviral therapy was consistent within the influenza groups (only oseltamivir was used n = 366), antiviral treatment in COVID-19 patients varied (lopinavir/ritonavir n = 44/65.7%, hydroxychloroquine n = 18/26.7%, camostat n = 3/4.5%, lopinavir/ritonavir plus hydroxychloroquine n = 1/1.5%, lopinavir/ritonavir plus remdesivir n = 1/1.5%).
There was no statistically significant difference in the use of antibiotic treatment (COVID-19 32.4%, InA 42.9%, InfB 40.7%, p = 0.112).
Discussion
In this study, we compared data from patients with severe COVID-19 and InfA and InfB, showing much higher in-hospital mortality for COVID-19. When comparing the patients’ demographics and medical history it was noted that InfB patients were significantly older. There was no statistically significant age difference between the COVID-19 and InfA group. The COVID-19 group had fewer comorbidities. Differences between InfA and InfB are already described in detail elsewhere and will not be discussed here [17]. Time from symptom onset to hospitalization was significantly longer in COVID-19 than in Influenza. This is in accordance with observations demonstrating that some SARS-CoV-2 infected patients deteriorate in the second week following symptom onset [18,19,20].
Despite fewer comorbidities in the COVID-19 group, in-hospital mortality was much higher than in InfA or InfB (COVID-19 23.2%, InfA 5.6% and InfB 4.7%). During the time this study was conducted, there was no shortage of ICU beds or healthcare system overburden in Austria. The department for infectious diseases was additionally equipped with further AIRVO™ 2 humidification systems at the start of the pandemic to offer high-flow nasal oxygen therapy for patients on the normal ward which could have prevented ICU admissions. This was not the case during previous influenza virus epidemics. Other than that quality of medical care and therapeutic options was identical and, therefore, this should not have had a negative effect on COVID-19 in-hospital mortality. In accordance with latest scientific findings at the time COVID-19 patients were treated with lopinavir/ritonavir or hydroxychloroquine as off-label therapy if they met certain severity and safety criteria, while a higher proportion of influenza patients received specific antiviral treatment (Oseltamivir). Low-molecular-weight-heparin was given to all patients without contraindication for thromboembolic prophylaxis in all study groups. At the time of the study data regarding therapy was scarce and dexamethasone, tocilizumab, remdesivir, APN01 and convalescent plasma were only used at the ICU as part of clinical trials. In a further analysis different age groups were compared. In-hospital mortality is higher in the COVID-19 group in all age groups above the age of 60 years, and while older age is a well-described risk factor for all of the studied viral infections [19, 21] differences in mortality increase dramatically with older age (see Table 3 and Fig. 3). While InfA and InfB in-hospital mortality increased moderately when comparing age groups 61–70 years and 81–90 years this was much more pronounced in COVID-19. Older age is already described as a major risk factor for COVID-19 but seems to be of greater importance than in other viral infections [19, 20, 22] Possible explanations include immunosenescence and decreased immune responses for this novel coronavirus as opposed to immunological memory to previous antigen exposure in the case of influenza (original antigenic sin) [23, 24]. We did not collect data on influenza vaccinations which may have prevented additional deaths in older patients with influenza.
While in-hospital mortality for influenza is widely known and accepted, recent publications demonstrate a significant increase when looking at 90-day mortality [25]. There is no information yet regarding long-term effects of COVID-19 or whether 30-day or 90-day mortality might be even higher than previously thought.
Excess mortality is an important endpoint to measure the impact of diseases or other environmental phenomena on a large scale. While seasonal excess mortality associated with influenza seasons is well-acknowledged [7] data for the current pandemic only became available recently. Concerns arose that under-treatment of other medical issues and delay of urgent medical procedures might lead to increased non-COVID-19-related mortality. Recent data demonstrates a significant rise in excess mortality for Europe after the seasonal influenza epidemic during the time of the SARS-CoV-2 pandemic. This excess mortality is driven solely by countries with high numbers of COVID-19 cases. In Austria, where a strict and early containment strategy was practiced no excess mortality was observed [26].
ICU admission rate did not differ in patients under 60 years of age. In the age group 61–70 years ICU admission rate was higher in the COVID-19 and InfA group. In addition, in the age group 71–80 years ICU admission was more common for COVID-19. In the COVID-19 group no patient older than 80 years was transferred to the ICU. Patients 80 years or older could either be managed with high-flow nasal oxygen therapy on the normal ward or ICU treatment was deemed to be non-beneficial for the patient due to comorbidities. Some patients also rejected ICU treatment on a personal decision. Transfer to ICU was not limited by availability during the pandemic in Austria. At our hospital the availability of high-flow oxygen on the normal ward did certainly reduce the number of ICU admissions. Unfortunately, as a downside of the fast and unbureaucratic initiation of high-flow oxygen on the normal ward as a response to the pandemic the documentation of high-flow oxygen usage was not standardized at the beginning and reliable interpretation to which extend this effected ICU admissions can therefore not be made.
Of interest, men seemed to be disproportionately affected with COVID-19 as compared to patients hospitalized with Influenza. Higher rates of COVID-19-associated morbidity and mortality in men versus women were reported previously and could potentially be explained by higher prevalence of smoking and alcohol consumption as well as other comorbidities in men compared to women. However, no such difference was observed in Influenza. Among other factors, different expression patterns between men and women of the viral receptors for SARS-CoV2 but not for Influenza may explain these differences [27, 28].
Alongside the higher mortality rate in COVID-19 other complications also appear to be more common. There was a significantly higher incidence of respiratory insufficiency, pneumonia, acute kidney injury and acute heart failure, as well as a significantly longer LOS which increases cost and burden on healthcare systems. The median time to patients being discharged from hospital is almost double for COVID-19 patients when compared to those with InfA and InfB (12 days vs 7 days respectively). The longer LOS might be partially explained due to hygienic reasons. At the beginning of the pandemic isolation of potentially infectious patients was particularly strict and two negative SARS-CoV-2 nasopharyngeal swaps have been necessary to end quarantine. Although people could theoretically have been discharged into self-quarantine at home or send to special “isolation-centers” this regularly delayed discharge, especially in people who needed personal assistance with activities of daily life. LOS for COVID-19 patients should be re-evaluated in further studies as rules for quarantine have changed considerably with increased knowledge about infectiousness and transmission of SARS-CoV-2 and adaption of care facilities to the challenges of the SARS-CoV-2 pandemic. Acute kidney injury was mostly mild and dialysis was not necessary in any patients on the normal ward, both in influenza patients as well as in COVID-19 patients. Organ replacement therapy as well as vasopressor use at the ICU were not analyzed in this study.
Laboratory results differed significantly, but differentiation based on laboratory results is not possible. Most notable in our opinion is the higher C-reactive protein (CRP) level accompanied by a lower leucocyte count. This supports our clinical impression of high CRP levels in COVID-19 with viral origin while bacterial superinfections seem rare [20]. In InfA and InfB high CRP levels are often associated with bacterial superinfections [29,30,31]. Unfortunately, we were unable to compare lymphocyte counts and other laboratory results associated with bad prognosis in COVID-19 due to missing values in our influenza A and B data set.
The strength of our study is that all patients had PCR-proven infections and were treated at the same department for infectious diseases by the same specialists, therefore, complications and in-hospital mortality could not have been influenced by different quality of healthcare or differences in expertise. The associated ICU was also managed by the same department. Successful containment strategies in Austria prevented ICU shortage during the time the data were collected which could have had an effect on mortality. To date, data comparing COVID-19, InfA and InfB in an elderly hospitalized population is scarce.
The retrospective collection of some of the data is a limitation of our study. The age group-specific mortality estimates may be biased by the small sample size within some subgroups. Data were collected at a single institution and findings might not be applicable to other settings. Furthermore, this study only represents COVID-19 patients during the “first wave” in Austria. During the course of the pandemic management of COVID-19 patients, therapeutic options, vaccination rollout, public restrictions and behavior as well as mutations of the virus changed continuously and will continue doing so. The impact of these factors on public health systems, illness presentation and course as well as on demographic changes of COVID-19 patients is of great interest and needs continuous analysis and interpretation.
In conclusion we could demonstrate the severity and high in-hospital mortality of COVID-19 in comparison to influenza A and influenza B. This result is supported by the excess mortality during the current SARS-CoV-2 pandemic in countries with a high disease burden. A higher reproduction number [3], more severe disease, longer LOS, insufficient therapeutic options and lack of vaccination for COVID-19 supports the strict containment policies practiced by most authorities, and renders the comment “it’s only flu”, which is sometimes used to trivialize the current pandemic, invalid.
References
- 1.
COVID-19 Dashboard. Available at: https://coronavirus.jhu.edu/map.html. Accessed 9 December 2020
- 2.
Fernandes N. Economic effects of coronavirus outbreak (COVID-19) on the world economy. Available at https://ssrn.com/abstract=3557504. Accessed 20 July 2020
- 3.
Riou J, Althaus CL. Pattern of early human-to-human transmission of Wuhan 2019 novel coronavirus (2019-nCoV), December 2019 to January 2020. Euro Surveill. 2020;25:2000058. https://doi.org/10.2807/1560-7917.ES.2020.25.4.2000058 (Published correction appears in Euro Surveill. 2020 Feb; 25(7)).
- 4.
Sanche S, Lin YT, Xu C, Romero-Severson E, Hengartner N, Ke R. High contagiousness and rapid spread of severe acute respiratory syndrome coronavirus 2. Emerg Infect Dis. 2020;26:1470–7. https://doi.org/10.3201/eid2607.200282.
- 5.
Biggerstaff M, Cauchemez S, Reed C, Gambhir M, Finelli L. Estimates of the reproduction number for seasonal, pandemic, and zoonotic influenza: a systematic review of the literature. BMC Infect Dis. 2014;14:480. https://doi.org/10.1186/1471-2334-14-480 (Published 2014 Sep 4).
- 6.
Iuliano AD, Roguski KM, Chang HH, et al. Estimates of global seasonal influenza-associated respiratory mortality: a modelling study. Lancet. 2018;391:1285–300. https://doi.org/10.1016/S0140-6736(17)33293-2 (Published correction appears in Lancet. 2018 Jan 19).
- 7.
Zucs P, Buchholz U, Haas W, Uphoff H. Influenza associated excess mortality in Germany, 1985–2001. Emerg Themes Epidemiol. 2005;2:6. https://doi.org/10.1186/1742-7622-2-6.
- 8.
Sanders JM, Monogue ML, Jodlowski TZ, Cutrell JB. Pharmacologic treatments for coronavirus disease 2019 (COVID-19): a review. JAMA. 2020. https://doi.org/10.1001/jama.2020.6019.
- 9.
Cao B, Wang Y, Wen D, et al. A trial of lopinavir-ritonavir in adults hospitalized with severe COVID-19. N Engl J Med. 2020;382:1787–99. https://doi.org/10.1056/NEJMoa2001282.
- 10.
Horby P, Lim WS, Emberson J, et al. Dexamethasone in hospitalized patients with COVID-19–preliminary report. N Engl J Med. 2020. https://doi.org/10.1056/NEJMoa2021436 (published online ahead of print, 2020 Jul 17).
- 11.
Mizumoto K, Kagaya K, Zarebski A, Chowell G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Euro Surveill. 2020;25:2000180. https://doi.org/10.2807/1560-7917.ES.2020.25.10.2000180.
- 12.
Day M. COVID-19: identifying and isolating asymptomatic people helped eliminate virus in Italian village. BMJ. 2020;368:m1165. https://doi.org/10.1136/bmj.m1165 (Published 2020 Mar 23).
- 13.
Leung NH, Xu C, Ip DK, Cowling BJ. Review article: the fraction of influenza virus infections that are asymptomatic: a systematic review and meta-analysis. Epidemiology. 2015;26:862–72. https://doi.org/10.1097/EDE.0000000000000340.
- 14.
Wilson N, Kvalsvig A, Barnard LT, Baker MG. Case-fatality risk estimates for COVID-19 calculated by using a lag time for fatality. Emerg Infect Dis. 2020;26:1339–441. https://doi.org/10.3201/eid2606.200320.
- 15.
Baud D, Qi X, Nielsen-Saines K, Musso D, Pomar L, Favre G. Real estimates of mortality following COVID-19 infection. Lancet Infect Dis. 2020;20:773. https://doi.org/10.1016/S1473-3099(20)30195-X.
- 16.
Ruan S. Likelihood of survival of coronavirus disease 2019. Lancet Infect Dis. 2020;20:630–1. https://doi.org/10.1016/S1473-3099(20)30257-7 (Published correction appears in Lancet Infect Dis. 2020 Apr 6).
- 17.
Karolyi M, Pawelka E, Daller S, et al. Is there a clinical difference between influenza A and B virus infections in hospitalized patients?: Results after routine polymerase chain reaction point-of-care testing in the emergency room from 2017/2018. Wien Klin Wochenschr. 2019;131:362–8. https://doi.org/10.1007/s00508-019-1519-0.
- 18.
Chen S, Feng H, Huang S, et al. Time windows for predicting deterioration in COVID-19 patients (4/10/2020). Available at SSRN: https://ssrn.com/abstract=3576808. http://dx.doi.org/https://doi.org/10.2139/ssrn.3576808
- 19.
Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382:1708–20. https://doi.org/10.1056/NEJMoa2002032.
- 20.
Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–62. https://doi.org/10.1016/S0140-6736(20)30566-3 (Published correction appears in Lancet. 2020 Mar 28; 395(10229):1038).
- 21.
Mehra MR, Desai SS, Kuy S, Henry TD, Patel AN. Cardiovascular disease, drug therapy, and mortality in COVID-19. N Engl J Med. 2020;382:e102. https://doi.org/10.1056/NEJMoa2007621 (Retracted in: N Engl J Med. 2020 Jun 4).
- 22.
Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020. https://doi.org/10.1001/jama.2020.2648 (Published online ahead of print, 2020 Feb 24).
- 23.
Henry C, Palm AE, Krammer F, Wilson PC. From original antigenic sin to the universal influenza virus vaccine. Trends Immunol. 2018;39:70–9. https://doi.org/10.1016/j.it.2017.08.003.
- 24.
Zhang A, Stacey HD, Mullarkey CE, Miller MS. Original antigenic sin: how first exposure shapes lifelong anti-influenza virus immune responses. J Immunol. 2019;202:335–40. https://doi.org/10.4049/jimmunol.1801149.
- 25.
Pawelka E, Karolyi M, Daller S, et al. Influenza virus infection: an approach to identify predictors for in-hospital and 90-day mortality from patients in Vienna during the season 2017/18. Infection. 2020;48:51–6. https://doi.org/10.1007/s15010-019-01335-0.
- 26.
European mortality monitoring. Available at https.//www.euromomo.eu/. Accessed 20 July 2020.
- 27.
Chen J, Jiang Q, Xia X, et al. Individual variation of the SARS-CoV-2 receptor ACE2 gene expression and regulation. Aging Cell. 2020. https://doi.org/10.1111/acel.13168.
- 28.
Culebras E, Hernández F. ACE2 is on the X chromosome: could this explain COVID-19 gender differences? Eur Heart J. 2020. https://doi.org/10.1093/eurheartj/ehaa521 (published online ahead of print, 2020 Jun 24).
- 29.
Ingram PR, Inglis T, Moxon D, Speers D. Procalcitonin and C-reactive protein in severe 2009 H1N1 influenza infection. Intensive Care Med. 2010;36:528–32. https://doi.org/10.1007/s00134-009-1746-3.
- 30.
von Baum H, Schweiger B, Welte T, et al. How deadly is seasonal influenza-associated pneumonia? The german competence network for community-acquired pneumonia. Eur Respir J. 2011;37:1151–7. https://doi.org/10.1183/09031936.00037410.
- 31.
Metersky ML, Masterton RG, Lode H, File TM Jr, Babinchak T. Epidemiology, microbiology, and treatment considerations for bacterial pneumonia complicating influenza. Int J Infect Dis. 2012;16:e321–31. https://doi.org/10.1016/j.ijid.2012.01.003.
- 1.



Πρόσφατα Σχόλια