Ο ΣΥΝΤΑΓΜΑΤΟΛΟΓΟΣ ΣΠΥΡΟΥ ΒΑΣΙΛΕΙΟΣ ΣΤΗΝ ΣΦΑΓΗ ΓΙΑ ΤΟΝ ΚΟΡΩΝΑΪΟ, ΜΑΣΚΑ, τον ΝΟΜΟ 4675 και 4682 κ.λπ. KAT΄ ΑΠΑΙΤΗΣΙΝ ΤΩΝ ΑΝΑΓΝΩΣΤΩΝ ΜΑΣ ΤΟ ΑΝΑΡΤΟΥΜΕ ΑΠΟ ΤΟ BRIGHΕTON
Ο συνταγματολόγος και κοινωνιλόγος, κ. Βασίλειος Σπύρου, μιλάει στην «ΣΦΑΓΗ» και στον Γιάννη Δεμερτζή για τα φλέγοντα θέματα της επικαιρότητας και όχι μόνο.
Πως στήσανε την γενοκτονία των Ελλήνων οι ξενόφερτοι πολιτικοί, για το μεγάλο πρόβλημα με τα σχέδια για την απαγωγή των παιδιών μας, με το πρόσχημα της ψεύτικης πανδημίας του Κορωναϊού, αλλά και άλλα θέματα, χρήσιμα για τον Έλληνα, έτσι ώστε να καταλάβει τι έχει γίνει, αλλά και να πράξει σωστά, δίχως να πέσει σε παγίδες, που στήνουν παρακομματικές οργανώσεις, αλλά και σύγχρονοι δωσίλογοι, για να οδηγήσουν στην τελική καταστροφή και στον αφανισμό, το Ελληνικό Γένος.
*Επειδή μας διαγράψαν το κανάλι, στο Youtube, στο οποίο είχαμε ανεβασμένο το βίντεο με τον κ. Σπύρου, σας έχουμε βάλει την νεότερη συνέντευξη παρακάτω, στο κανάλι της «ΣΦΑΓΗΣ», στο Brighteon !
Αποκαλύψεις που συγκλονίζουν: Ποιοι, πώς και γιατί δημιούργησαν τον Covid-19 – O ρόλος Ελλήνων επιστημόνων
Σε πλήρη εξέλιξη βρίσκονται σε όλο τον κόσμο έρευνες της Δικαιοσύνης και των αστυνομικών αρχών των κατά τόπους χωρών προκειμένου να ξεσκεπαστεί η συνωμοσία που στήθηκε προκειμένου για τον ύποπτο ρόλο του ζωολόγου Peter Daszak, προέδρου της EcoHealth Alliance, η οποία χρηματοδότησε την συγκάλυψη της έρευνας για την προέλευση του κορωνοϊού εμπλέκοντας μάλιστα και Έλληνες επιστήμονες σε αυτή την συγκάλυψη: Τα ονόματα των S. Tsiodras, G. Magiorkinis, D. Paraskevis, E.G. Kostaki, G. Panayiotakopoulos, φιγουράρουν στην «επιστημονική μελέτη» με τίτλο «Full-genome evolutionary analysis of the novel corona virus (2019-nCoV) rejects the hypothesis of emergence as a result of a recent recombination event» στις 27 Ιανουαρίου 2020 στο biorxiv.org, ένα «αποθετήριο μελετών» που χρηματοδοτήθηκε από τον Zuckerberg του Facebook με αρκετά εκατομμύρια δολάρια.
Η συγκεκριμένη «μελέτη» ήρθε στην δημοσιότητα στην Ελλάδα όταν στις 30 Ιανουαρίου 2020 η ΚΑΘΗΜΕΡΙΝΗ προέβαλε την μελέτη γράφοντας: «Ερευνητές του ΕΚΠΑ και του Πανεπιστημίου Κρήτης, μελετώντας τα γενετικά χαρακτηριστικά του νέου ιού απέκλεισαν το ενδεχόμενο αυτός να προέρχεται από ερπετά, ενώ κατέληξαν στο συμπέρασμα ότι πρόκειται για ένα νέο για τον άνθρωπο κορωνοϊό και όχι αποτέλεσμα πρόσφατης γενετικής ανάμειξης με άλλον ιό της ίδιας “οικογένειας”».
Τι έλεγε εκείνη η «μελέτη»; Ότι ο Covid-19 είχε γεννηθεί από την φύση και μεταδόθηκε στους ανθρώπους που έτρωγαν νυχτερίδες από την κρεαταγορά της Ουχάν, αθωώνοντας πλήρως τα κινεζικά βιολογικά εργαστήρια που έτσι ή αλλιώς εκτελούσαν παραγγελία από κύκλους των… ΗΠΑ!
Τότε μπορεί να μην τους ήξερε η πλειοψηφία των Ελλήνων αλλά στην πανεπιστημιακή κοινότητα της ιατρικής, ήταν γνωστοί: Αναπληρωτής καθηγητής ο Δημήτριος Παρασκευής, και η η Ευαγγελία-Γεωργία Κωστάκη, ο επίκουρος καθηγητής ο Γκίκας Μαγιορκίνης από το Εργαστήριο Υγιεινής Επιδημιολογίας και Ιατρικής Στατιστικής του ΕΚΠΑ, επίκουρος καθηγητής και αντιπρόεδρος του ΕΟΔΥ ο Γεώργιος Παναγιωτακόπουλος, καθηγητής κλινικής ιολογίας του Πανεπιστημίου Κρήτης και μέλος ΔΣ του ΕΟΔΥ ο Γεώργιος Σουρβίνος και βέβαια, πάνω απ’όλους ο καθηγητής Παθολόγος – Λοιμωξιολόγος Σωτήρης Τσιόδρας.
Τότε δεν ήταν αστέρια της τηλεόρασης, αλλά αυτό δεν τους εμπόδισε να αναπτύξουν θεωρίες που στήριζε το ίδρυμα EcoHealth Alliance: Ότι ο Covid-19 ήταν προϊόν της φύσης και όχι των βιολογικών εργαστηρίων της Ουχάν.
Δηλαδή οι άνθρωποι υπέγραψαν μία μελέτη που τους παραγγέλθηκε και κατέληξαν από χιλιάδες χιλιόμετρα μακριά σε ασφαλές συμπέρασμα ότι ο ιός είναι αποτέλεσμα φυσικών διαδικασιών!
Ως να είχαν γνώση μεθόδων και τεχνικών βιολογικού πολέμου και «γενετικού μαγειρέματος» ιών.
Η μελέτη των προαναφερθέντων Ελλήνων «ειδικών» λειτούργησε ως τμήμα του μηχανισμού από τον Peter Daszak της EcoHealth Alliance, συνεργάτη του Ιδρύματος Gates, επιθεωρητής-συνεργάτης του Παγκόσμιου Οργανισμού Υγείας και συνεργάτης των αμερικανικών Ενόπλων Δυνάμεων, για να κατασκευάσει «επιστημονική τεκμηρίωση» ότι ο ιός μόλυνε τον άνθρωπο με φυσικές διαδικασίες και ότι ο SARS-CoV2, ο ιός που προκαλεί την COVID-19, προέκυψε με φυσικό τρόπο από μια κρεαταγορά της Ουχάν.
Οι έρευνες των αρχών τεκμηριώνουν σταδιακά την απάντηση στο ερώτημα «Πώς αποκτήσαμε μια επιστημονική και μιντιακή συναίνεση ότι ο SARS-CoV2 προήλθε εξ’ αρχής από την κρεαταγορά της Ουχάν;».
Και η πρώτη απάντηση δίνεται από την περίφημη ομαδική επιστολή υπογεγραμμένη από κορυφαίους επιστήμονες που εμφανίστηκε στην αξιόπιστη επιστημονική έκδοση The Lancet (https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30418-9/fulltext).
Ουσιαστικά, οι Αμερικανοί (της κυβέρνησης Ομπάμα) προσπάθησαν να καλύψουν ότι αυτοί είχαν χρηματοδοτήσει τα κινεζικά εργαστήρια (το παραδέχθηκε και ο Fauci σε βάρος του οποίου διεξάγεται τώρα έρευνα από την αμερικανική Γερουσία για τον λόγο αυτό). Η έρευνα χρηματοδοτήθηκε από το Εθνικό Ινστιτούτο Αλλεργιών και Λοιμωδών Νόσων του Δρ. Anthony Fauci!
Ο Daszak συνεργάστηκε με τον Ralph Baric του Πανεπιστημίου της Βόρειας Καρολίνας και ο όμιλος του Daszak, η EcoHealth Alliance, συνεργάστηκε απευθείας με τα εργαστήρια της Κίνας στην Wuhan για να ερευνήσει κορωνοϊούς και δυνητικά να τούς κάνει περισσότερο μεταδοτικούς και περισσότερο θανατηφόρους.
Όταν ο Daszak έμαθε ότι ένας ιός από το συγκεκριμένο εργαστήριο είχε «δραπετεύσει» και προκαλούσες εν δυνάμει παγκόσμια καταστροφή, κινήθηκε γρήγορα ώστε να ευθυγραμμίσει την επιστημονική κοινότητα για να δηλώσουν, χωρίς καμία πειστική απόδειξη, ότι ο COVID-19 είχε «φυσική προέλευση».
Και η μελέτη των Ελλήνων «ειδικών», που αναφέρεται βιβλιογραφικά στην επιστολή στο Lancet, φαίνεται να εξυπηρέτησε την κατασκευή κλίματος για αντιεπιστημονική ευθυγράμμιση επιστημόνων σε απόκρυψη πιθανού εγκλήματος και σε κάλυψη των ευθυνών του Daszak και του χώρου αμερικανικών κυβερνητικών Υπηρεσιών γύρω του.
Πλέον είναι βέβαιο ότι βάσει μηνυμάτων ηλεκτρονικού ταχυδρομείου που ελήφθησαν από μια ομάδα ελευθερίας πληροφοριών που ονομάζεται «ΗΠΑ Δικαίωμα Γνώσης», ότι ο Daszak όχι μόνο τελικά υπέγραψε, αλλά οργάνωσε την δήλωση επιρροής στο Lancet με την συμμετοχή και των Ελλήνων επιστημόνων, με την πρόθεση να κρύψει τον ρόλο του στη ανάπτυξη του Covid-19 και να δημιουργήσει την εντύπωση της επιστημονικής ομοφωνίας για την προέλευση του Covid-19.
Ο Daszak κινητοποιήθηκε τόσο γρήγορα για έναν λόγο, είπε ο Jamie Metzl: «Αν η πανδημία ξεκίνησε ως μέρος μιας εργαστηριακής διαρροής, είχε τη δυνατότητα να κάνει στην Ιολογία αυτό που έκανε το Three Mile Island και το Chernobyl στην πυρηνική επιστήμη: Θα μπορούσε να χτυπήσει τον τομέα επ’ αόριστον με μορατόριουμ και περιορισμούς χρηματοδότησης»!
Άρα πέρα από την απόσειση των ποινικών ευθυνών υπήρχε και οικονομικό θέμα: Θα έχαναν τις επιδοτήσεις!
Σύμφωνα με βίντεο που ανακαλύφθηκε από το The National Pulse ο Daszak φαίνεται να καυχιέται για τη χειραγώγηση των «δολοφόνων» κορωνοϊών που μοιάζουν με SARS.
Ο Daszak προέβη σε αυτήν την παραδοχή σε ένα φόρουμ του 2016, συζητώντας για «αναδυόμενες μολυσματικές ασθένειες και την επόμενη πανδημία», το οποίο φαίνεται να έρχεται σε αντίθεση με την επανειλημμένη άρνηση του Fauci να χρηματοδοτήσει έρευνα στο Ινστιτούτο ιολογίας του Γουχάν.
Ενώ περιγράφει τον τρόπο με τον οποίο η οργάνωσή του ακολουθεί θανατηφόρους ιούς, ο Daszak περιγράφει τη διαδικασία «εισαγωγής [spike protein] σε ιούς για να δουν αν μπορούν να συνδεθούν με ανθρώπινα κύτταρα όπως πραγματοποιούνται από τους συναδέλφους του στην Κίνα»!
Λέει ακριβώς: «Βρήκαμε άλλους κορωνοϊούς σε νυχτερίδες, ένα πλήθος από αυτούς, μερικοί από αυτούς έμοιαζαν πολύ παρόμοιοι με το SARS. Έτσι, ακολουθήσαμε την αλληλουχία της ακίδα πρωτεΐνης: της πρωτεΐνης που προσκολλάται στα κύτταρα. Λοιπόν, δεν έκανα εγώ αυτό το έργο, αλλά οι συνάδελφοί μου στην Κίνα έκαναν τη δουλειά.
Δημιουργείτε ψευδο-σωματίδια, εισάγετε τις ακίδες πρωτεΐνες από αυτούς τους ιούς, βλέπετε αν συνδέονται με ανθρώπινα κύτταρα.
Σε κάθε βήμα αυτού, προχωράτε πιο κοντά σε αυτόν τον ιό που θα μπορούσε πραγματικά να γίνει παθογόνος στους ανθρώπους. Καταλήγεις με έναν μικρό αριθμό ιών που μοιάζουν πραγματικά με δολοφόνους»!
Τα σχόλια ακολουθούν αυξανόμενες ενδείξεις ότι το Εθνικό Ινστιτούτο Αλλεργίας και Λοιμωδών Νοσημάτων (NIAID) του Fauci έχει βαθιές οικονομικές σχέσεις με το Ινστιτούτο ιολογίας του Wuhan και ότι η EcoHealth του Daszak ήταν ένας από τους κύριους αντιπροσώπους που διοχετεύουν τα χρήματα στο εργαστήριο του Κομμουνιστικού Κόμματος της Κίνας.
Πάνω από δώδεκα ερευνητικές εργασίες που εκπονήθηκαν στο πλαίσιο επιχορήγησης του Εθνικού Ινστιτούτου Αλλεργίας και Λοιμωδών Νοσημάτων (NIAID) 3,7 εκατομμυρίων δολαρίων, αναφέρουν την διευθύντρια του Κέντρου Αναδυόμενων Λοιμωδών Νοσημάτων του εργαστηρίου του Wuhan, Shi Zhengli ως συν-συγγραφέα μαζί με τον Daszak. Η Σι έχει συμπεριλάβει αυτές τις επιχορηγήσεις με υποστήριξη Fauci στο βιογραφικό της.
Όχι μόνο ο Daszak ενορχήστρωσε την σύνταξη και το κείμενο της επιστολής που συνυπέγραψαν και οι Έλληνες επιστήμονες στο Lancet, αλλά το έκανε, σύμφωνα με το Vanity Fair, «με την πρόθεση να κρύψει τον ρόλο του και να δημιουργήσει την εντύπωση της επιστημονικής ασυλίας».
Μάλιστα σε ένα από τα email που διέρρευσαν ο ο Daszak απευθύνεται στον Baric, και του λέει: «Δεν χρειάζεται να υπογράψεις την “Δήλωση” Ralph για να φανεί ότι έχει κάποια απόσταση από εμάς και ως εκ τούτου να μην λειτουργεί με αντιπαραγωγικό τρόπο. Στη συνέχεια θα το βγάλουμε με τρόπο που δεν θα το συνδέεται με τη συνεργασία μας, έτσι μεγιστοποιούμε μια ανεξάρτητη φωνή»!
Ο Baric συμφώνησε, απαντώντας,
«Διαφορετικά φαίνεται ως αυτοεξυπηρέτηση και χάνουμε τον αντίκτυπο»!
Όμως άλλοι έξι από αυτούς που υπέγραψαν την δήλωση είτε εργάστηκαν είτε είχαν λάβει χρηματοδότηση από την EcoHealth Alliance, σύμφωνα με το Vanity Fair.
Σε ένα βίντεο που λήφθηκε αρχικά στις 9 Δεκεμβρίου 2019, τρεις εβδομάδες πριν από την ανακοίνωση της Δημοτικής Επιτροπής Υγείας της Wuhan μιας νέας μορφής πνευμονίας, ο ιολόγος Vincent Racaniello πήρε συνέντευξη από τον Βρετανό ζωολόγο και πρόεδρο της EcoHealth Alliance Peter Daszak για το έργο του στο μη κερδοσκοπικό οργανισμό για την προστασία του κόσμου από την εμφάνιση νέων ασθενειών και την πρόβλεψη πανδημιών.
Επείγουσα βρετανική έκθεση ζητά άμεση διακοπή όλων των εμβολιασμών COVID
Μια “επείγουσα προκαταρκτική έκθεση των δεδομένων της Κίτρινης Κάρτας” που εκδόθηκε από την εταιρεία Evidence-Based Medicine Consultancy Ltd με έδρα το Ηνωμένο Βασίλειο και υποβλήθηκε στην Υπηρεσία Ρύθμισης Φαρμάκων και Προϊόντων Υγείας (MHRA) αναφέρει ότι “η MHRA έχει πλέον περισσότερα από αρκετά στοιχεία από το σύστημα της Κίτρινης Κάρτας (Yellow Card) για να κηρύξει τα εμβόλια COVID-19 μη ασφαλή για χρήση στον άνθρωπο”.Όπως το Αμερικανικό Σύστημα Αναφοράς Ανεπιθύμητων Συμβάντων από Εμβόλια (VAERS), η MHRA περιγράφει τον σκοπό του συστήματος της Κίτρινης Κάρτας ως μια “έγκαιρη προειδοποίηση ότι η ασφάλεια ενός φαρμάκου ή ενός ιατροτεχνολογικού προϊόντος μπορεί να απαιτεί περαιτέρω διερεύνηση”.
Η έκθεση, η οποία υπογράφεται από την Διευθύντρια της Evidence-based Medicine Consultancy Ltd και της EbMC Squared CiC, Δρ. Tess Lawrie (MBBCh, PhD), αναφέρει: “πραγματοποιήσαμε αναζήτηση στις εκθέσεις της Κίτρινης Κάρτας χρησιμοποιώντας λέξεις – κλειδιά που αφορούν την παθολογία για να ομαδοποιήσουμε τα δεδομένα σύμφωνα με τις ακόλουθες πέντε [sic] ευρείες, κλινικά σχετικές κατηγορίες:
Αιμορραγία, πήξη και ισχαιμικές ανεπιθύμητες ενέργειες
Αντίδραση στο ανοσοποιητικό σύστημα
Αντίδραση από πόνο
Νευρολογικές ανεπιθύμητες ενέργειες
Αντίδραση που συνεπάγεται απώλεια της όρασης, της ακοής, της ομιλίας ή της όσφρησης
Ανεπιθύμητες ενέργειες εγκυμοσύνης”
Η έκθεση συνεχίζει λέγοντας: «Γνωρίζουμε τους περιορισμούς των δεδομένων φαρμακοεπαγρύπνησης και κατανοούμε ότι οι πληροφορίες σχετικά με τις αναφερθείσες ανεπιθύμητες ενέργειες δεν πρέπει να ερμηνεύονται ως ένδειξη ότι το εν λόγω φάρμακο προκαλεί γενικά το παρατηρούμενο αποτέλεσμα ή ότι δεν είναι ασφαλές για χρήση. Κοινοποιούμε αυτή την προκαταρκτική έκθεση λόγω της επείγουσας ανάγκης να κοινοποιήσουμε πληροφορίες που θα πρέπει να οδηγήσουν στην παύση της εφαρμογής του εμβολιασμού, ενώ διεξάγεται πλήρης έρευνα. Σύμφωνα με την πρόσφατη δημοσίευση των Seneff και Nigh, οι πιθανές οξείες και μακροχρόνιες παθολογικές καταστάσεις περιλαμβάνουν:
Παθογενετική προετοιμασία, πολυσυστημική φλεγμονώδης νόσος και αυτοανοσία
Αλλεργικές αντιδράσεις και αναφυλαξία
Εξαρτώμενη από τα αντισώματα ενίσχυση
Ενεργοποίηση λανθάνουσας ιογενούς λοίμωξης
Νευροεκφυλισμός και ασθένειες prion
Ανάδυση νέων παραλλαγών του SARSCoV2
Ενσωμάτωση του γονιδίου της πρωτεΐνης spike στο ανθρώπινο DNA»
«Είναι πλέον προφανές ότι τα προϊόντα αυτά στην κυκλοφορία του αίματος είναι τοξικά για τον άνθρωπο. Απαιτείται η άμεση διακοπή του προγράμματος εμβολιασμού, ενόσω διεξάγεται πλήρης και ανεξάρτητη ανάλυση ασφάλειας για τη διερεύνηση της πλήρους έκτασης των βλαβών, οι οποίες σύμφωνα με τα στοιχεία της Κίτρινης Κάρτας του Ηνωμένου Βασιλείου περιλαμβάνουν θρομβοεμβολισμό, φλεγμονώδη νόσο πολλαπλών συστημάτων, ανοσοκαταστολή, αυτοανοσία και αναφυλαξία, καθώς και ενίσχυση εξαρτώμενη από αντισώματα (ADE).»
Η έκθεση καταλήγει: «Η MHRA διαθέτει πλέον περισσότερα από αρκετά στοιχεία από το σύστημα Κίτρινης Κάρτας για να κηρύξει τα εμβόλια COVID-19 μη ασφαλή για χρήση στον άνθρωπο. Θα πρέπει να γίνει προετοιμασία για την κλιμάκωση των ανθρωπιστικών προσπαθειών προκειμένου να βοηθηθούν όσοι έχουν υποστεί βλάβη από τα εμβόλια COVID-19 και να προβλεφθούν και να βελτιωθούν οι μεσοπρόθεσμες και μακροπρόθεσμες επιπτώσεις. Δεδομένου ότι ο μηχανισμός των βλαβών από τα εμβόλια φαίνεται να είναι παρόμοιος με τον ίδιο τον COVID-19, αυτό περιλαμβάνει τη συνεργασία με πολυάριθμους διεθνείς γιατρούς και επιστήμονες με εμπειρία στην επιτυχή θεραπεία του COVID-19.
Υπάρχουν τουλάχιστον 3 επείγοντα ερωτήματα που πρέπει να απαντηθούν από την MHRA:
1. Πόσοι άνθρωποι έχουν πεθάνει εντός 28 ημερών από τον εμβολιασμό;
2. Πόσοι άνθρωποι έχουν νοσηλευτεί σε νοσοκομείο εντός 28 ημερών από τον εμβολιασμό;
3. Πόσοι άνθρωποι έχουν μείνει ανάπηροι από τον εμβολιασμό;»
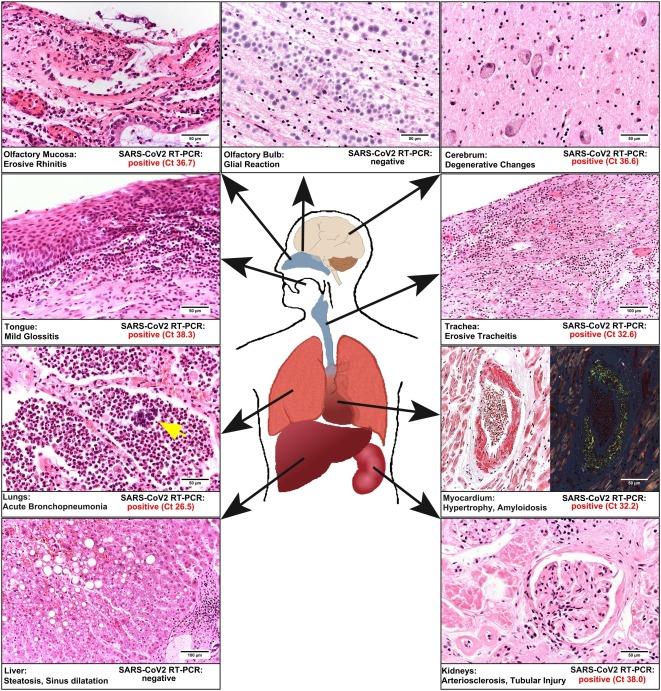
Πρώτη μεταθανάτια μελέτη σε εμβολιασμένο ασθενή κατά Covid19 δείχνει ότι όλα τα όργανα του είχαν μολυνθεί με πρωτεΐνες Spike, το ιικό RNA ήταν σε όλα τα όργανά του!!
H 1η μελέτη επί αυτοψίας νεκρού εμβολιασμένου κατά του covid αποκάλυψε ότι το ιικό RNA βρέθηκε σε κάθε όργανο του σώματος του ασθενούς, πράγμα που σημαίνει ότι το εμβόλιο είναι είτε αναποτελεσματικό είτε ο κορωναϊός εξαπλώνεται πιο γρήγορα σε εμβολιασμένα άτομα.
Eίχε υποβληθεί σε τεστ που αποδείχθηκε αρνητικό 18 μέρες πιο αργά κατά την εισαγωγή του στο νοσοκομείο αλλά 24 ώρες μετά τον εμβολιασμό του αποκαλύφθηκε ότι το ιικό RNA ήταν παρόν σχεδόν σε όλα τα όργανά του σώματός του. Το εμβόλιο προκάλεσε μια ανοσοποιητική αντίδραση δεν εμπόδισε τον ιό να εισχωρήσει σε όλα τα όργανα του σώματός του. Το ιικό RNA ανιχνεύθηκε σχεδόν σε όλα τα όργανα του σώματός του κάτι που σημαίνει ότι επίσης και οι πρωτείνες Spike.
Σύμφωνα με τη δημοσιευμένη έκθεση αυτοψίας, ο εμβολιασμένος άνδρας ήταν 86 ετών και υποβλήθηκε σε τεστ για COVID-19 που αποδείχθηκε αρνητικό όταν εισήχθη στο νοσοκομείο με σοβαρά γαστρεντερικά προβλήματα και δυσκολίες στην αναπνοή. Αυτό περιγράφει η έκθεση:
Αναφέρεται η περίπτωση ενός 86χρονου άνδρα τροφίμου σε Οίκο Ευγηρίας που έλαβε το εμβόλιο κατά SARS-CoV-2. Το ιατρικό ιστορικό του περιελάμβανε συστηματική υπέρταση, χρόνια φλεβική ανεπάρκεια, άνοια και καρκίνωμα του προστάτη. Στις 9 Ιανουαρίου 2021, ο άνδρας έλαβε το εμβόλιο mRNA με νουκλεοζίτη BNT162b2 ως νανοσωματίδια λιπιδίων σε δόση 30 μg. Εκείνη την ημέρα και για τις επόμενες 2 εβδομάδες, δεν έδειξε κλινικά συμπτώματα (Πίνακας 1). Την 18η ημέρα εισήχθη στο νοσοκομείο με επιδείνωση της διάρροιας. Καθώς δεν έδειξε κλινικά συμπτώματα COVID-19, δεν υπήρξε απομόνωση του σε ένα συγκεκριμένο περιβάλλον. Οι εργαστηριακές εξετάσεις αποκάλυψαν υποχρωμική αναιμία και αυξημένα επίπεδα κρεατινίνης στον ορό. Το τεστ αντιγόνου και η αλυσιδωτή αντίδραση πολυμεράσης (PCR) για SARS-CoV-2 ήταν αρνητικά.
Η έκθεση αυτοψίας ανέφερε ότι οι εξετάσεις δεν έδειξαν «καμία μορφολογική αλλαγή που σχετίζεται με το COVID» στα όργανα του.
«Μορφολογική» σημαίνει δομική. Η μόλυνση με COVID είναι πλέον γνωστό ότι προκαλεί πολύ συγκεκριμένες δομικές αλλαγές στα μέρη που μολύνει. Αυτές οι αλλαγές δεν παρατηρήθηκαν στον εμβολιασμένο άνδρα πριν από το θάνατό του.
Ο πλέον νεκρός εμβολιασμένος άνδρας βρισκόταν σε ένα δωμάτιο όπου ένας άλλος ασθενής που ήταν τελικά θετικός σε COVID και η έκθεση αναφέρει ότι θεωρεί ότι ο νεκρός εμβολιασμένος άνδρας μολύνθηκε από COVID μετά την εισαγωγή του, από τον άλλο ασθενή στο ίδιο δωμάτιο.
Το χειρότερο είναι ότι όταν ο εμβολιασμένος άνδρας μολύνθηκε πραγματικά με COVID, αυτό εξαπλώθηκε στο σώμα του τόσο γρήγορα που προφανώς δεν είχε καμία πιθανότητα.Το ιικό RNA βρέθηκε σε κάθε όργανο του σώματος του.Πέθανε 4 εβδομάδες μετά τον εμβολιασμό του. Με μεταθανάτια μοριακή χαρτογράφηση, βρέθηκε ιικό RNA σε σχεδόν όλα τα όργανα του που εξετάστηκαν. Ωστόσο, δεν παρατηρήθηκε κανένα μορφολογικό χαρακτηριστικό του COVID-19.
Θα μπορούσε να προκληθεί ανοσογονικότητα, ενώ δεν έχει αποδειχθεί αποστειρωμένη ανοσία.
Συνοπτικά, αυτή η μελέτη, η οποία πρέπει να επιβεβαιωθεί από άλλους, προτείνει και δίνει τεκμήριο ότι 1 / το εμβόλιο RNA δεν προστατεύει
2 / το εμβόλιο επιταχύνει ή έχει τη δυνατότητα να επιταχύνει την εξάπλωση του ιού στο σώμα …
Το εμβόλιο, ενώ πυροδότησε μια ανοσολογική απόκριση, δεν εμπόδισε τον ιό να εισέλθει σε όλα τα όργανα του σώματος.
Υπάρχουν αντισώματα (όπως αυτά που υποτίθεται ότι δημιουργεί το “εμβόλιο”), αλλά είναι άσχετα επειδή, σύμφωνα με ιαπωνική μελέτη, γνωρίζουμε τώρα ότι είναι η πρωτεΐνη ακίδα S1 που προκαλεί τη βλάβη.
Το eveilhomme αναφέρει ότι μίλησε με έναν ειδικό για τις μολυσματικές ασθένειες σε νοσοκομείο του Νιου Τζέρσεϋ σήμερα το πρωί. ”Του στείλαμε τα αποτελέσματα της αυτοψίας και ζητήσαμε τη γνώμη του.
Όταν μας κάλεσε πίσω αργότερα, σαφώς κλονίστηκε. Μας είπε, “Δεν μπορείτε να με αναφέρετε με όνομα, θα απολυθώ από το νοσοκομείο εάν το κάνετε.” Συμφωνήσαμε να αποκρύψουμε την ταυτότητά του.”
Τότε μας είπε:
«Οι άνθρωποι πιστεύουν ότι μόνο μια μειονότητα ανθρώπων εμφανίζει παρενέργειες από το εμβόλιο.
Σύμφωνα με αυτή τη νέα έρευνα, αυτό σημαίνει ότι όλοι – τελικά – θα έχουν παρενέργειες, καθώς αυτές οι πρωτεΐνες Spike θα συνδέονται με τους υποδοχείς ACE2 σε όλο το σώμα.
Αυτό το mRNA έπρεπε να παραμείνει στο σημείο της ένεσης, αλλά δεν το κάνει. Αυτό σημαίνει ότι οι πρωτεΐνες Spike που δημιουργούνται από το mRNA θα βρεθούν επίσης σε όλα τα όργανα και τώρα γνωρίζουμε ότι οι πρωτεΐνες Spike προκαλούν τη βλάβη.
Ακόμη χειρότερα, η παρουσία ιικού RNA σε όλα τα όργανα, παρά το εμβόλιο, δείχνει:
1) Είτε το εμβόλιο δεν λειτουργεί καθόλου.
2) Είτε ο ιός επωφελείται από την ενίσχυση που εξαρτάται από αντισώματα (ADE), που σημαίνει ότι εξαπλώνεται ταχύτερα σε άτομα που έχουν εμβολιαστεί.
Αυτή είναι μια παγκόσμια ωρολογιακή βόμβα. “
ΟΛA ΣΤΟ ΦΩΣ🆘 ➡️Για ποιο λόγο πραγματικά μαγνητίζουν οι ενέσεις Φραγκεστάιν💉💉 📌Συνέντευξη του Stew Peters με τη Δρ Jane Ruby – Τεχνολογία Magnetofection
Είδαμε στο κανάλι ΑΡΤ τον τηλεπαρουσιαστή κ. Καμπούρη, μετά τον εμβολιασμό του, να κολλάει ένα τεράστιο ψαλίδι στο μπράτσο του που στερεώθηκε προφανώς λόγω μαγνητικής έλξης οφειλόμενης στο εμβόλιο που έκανε. Ο συγκεκριμένος τηλεπαρουσιαστής, το έπραξε αυτό, επειδή απλούστατα, όπως όλοι μας, είδε τα εκατοντάδες βίντεο που κυκλοφορούν στο διαδίκτυο δεχόμενα τον χλευασμό των “ειδικών” που έλεγαν ότι αυτά είναι παραμύθια και δεν ισχύει τίποτε από αυτά.
Μετά από το σοκαριστικό LIVE του ΑΡΤ, οι “ειδικοί” είπαν ότι το παράδοξο αυτό φαινόμενο, δεν εξηγείται ιατρικώς κάποιοι μάλιστα είπαν, ότι πρώτη φορά το βλέπουν (!!!!!!!) ενώ βοά ο πλανήτης ολόκληρος.
Τίθεται λοιπόν το μέγα ερώτημα:
ΤΙ ΑΛΛΟ ΔΕΝ ΞΕΡΟΥΝ ΓΙΑ ΤΑ ΕΜΒΟΛΙΑ COVID οι “ειδικοί” ;;;;;;;
Αν σου απαντήσουν να το αναφέρεις και στο διασυμπαντικό πλανητικό σύστημα!Πρέπει να σώσουμε τους Alliens από τους Χαζάρους γιατί είναι χαμένος κόπος να ασχοληθείς με τα ενδογήινα δίποδα ινδικά χοιρίδια-πειραματόζωα:
Χαμένος ο κόπος σου Φίλιππε αν περιμένεις από τη Λιανού, την Παγώνη, τον Τσιόδρα, τον Βασιλακόπουλο, τον Εξαδάκτυλο και όλο το εκλεκτό επιτελείο της ιατρικής επιτροπής για τον κοροϊδοϊό να σου εξηγήσουν τι συμβαίνει.
Δεν αντιλαμβάνεσαι ότι Κυβέρνηση και ιατρικό συνδικάτο μας έχουν βάλει για τα καλά σε έναν κόσμο τύπου Matrix;
Ένας εισαγγελέας έντιμος, ευσυνείδητος και με ηθικές ευαισθησίες δεν υπάρχει σ’ αυτόν τον ρημαγμένο τόπο;
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections and the resulting disease, coronavirus disease 2019 (Covid-19), have spread to millions of persons worldwide. Multiple vaccine candidates are under development, but no vaccine is currently available. Interim safety and immunogenicity data about the vaccine candidate BNT162b1 in younger adults have been reported previously from trials in Germany and the United States.
Methods
In an ongoing, placebo-controlled, observer-blinded, dose-escalation, phase 1 trial conducted in the United States, we randomly assigned healthy adults 18 to 55 years of age and those 65 to 85 years of age to receive either placebo or one of two lipid nanoparticle–formulated, nucleoside-modified RNA vaccine candidates: BNT162b1, which encodes a secreted trimerized SARS-CoV-2 receptor–binding domain; or BNT162b2, which encodes a membrane-anchored SARS-CoV-2 full-length spike, stabilized in the prefusion conformation. The primary outcome was safety (e.g., local and systemic reactions and adverse events); immunogenicity was a secondary outcome. Trial groups were defined according to vaccine candidate, age of the participants, and vaccine dose level (10 μg, 20 μg, 30 μg, and 100 μg). In all groups but one, participants received two doses, with a 21-day interval between doses; in one group (100 μg of BNT162b1), participants received one dose.
Results
A total of 195 participants underwent randomization. In each of 13 groups of 15 participants, 12 participants received vaccine and 3 received placebo. BNT162b2 was associated with a lower incidence and severity of systemic reactions than BNT162b1, particularly in older adults. In both younger and older adults, the two vaccine candidates elicited similar dose-dependent SARS-CoV-2–neutralizing geometric mean titers, which were similar to or higher than the geometric mean titer of a panel of SARS-CoV-2 convalescent serum samples.
Conclusions
The safety and immunogenicity data from this U.S. phase 1 trial of two vaccine candidates in younger and older adults, added to earlier interim safety and immunogenicity data regarding BNT162b1 in younger adults from trials in Germany and the United States, support the selection of BNT162b2 for advancement to a pivotal phase 2–3 safety and efficacy evaluation. (Funded by BioNTech and Pfizer; ClinicalTrials.gov number, NCT04368728. opens in new tab.)
Since the first cases of coronavirus disease 2019 (Covid-19) in Wuhan, China, in December 2019, pandemic illness has spread to millions of persons worldwide. An increased risk of severe disease and death has been noted among the elderly and among persons with preexisting medical conditions. No Covid-19 vaccines are currently available, and they are urgently needed to combat escalating cases and deaths worldwide.1
In response, BioNTech and Pfizer launched a coordinated program to compare four RNA-based Covid-19 pandemic vaccine candidates in umbrella-type clinical studies conducted in Germany (BNT162-01) and the United States (C4591001). The program was designed to support the selection of a single vaccine candidate and dose level for a pivotal international safety and efficacy trial. On the basis of initial clinical-trial results in Germany,2 two lipid nanoparticle–formulated,3 nucleoside-modified RNA (modRNA)4 vaccine candidates against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) were evaluated in the phase 1 portion of the trial in the United States.5 One of these candidates, BNT162b1, encodes the SARS-CoV-2 receptor–binding domain, trimerized by the addition of a T4 fibritin foldon domain to increase its immunogenicity through multivalent display.6-8 The other candidate, BNT162b2, encodes the SARS-CoV-2 full-length spike, modified by two proline mutations to lock it in the prefusion conformation9 and more closely mimic the intact virus with which the elicited virus-neutralizing antibodies must interact.10
Previous articles have described the assessment of BNT162b1, at multiple dose levels, in healthy adults 18 to 55 years of age.2,5 These studies indicated that dose levels of BNT162b1 that elicited an acceptable level of reactogenicity also efficiently elicited titers that were as high as those in a panel of SARS-CoV-2 human convalescent serum samples and that were broadly neutralizing across a panel of 17 SARS-CoV-2 pseudoviruses representing a diversity of circulating strains. BNT162b1 also elicited CD4+ type 1 helper T (Th1) cell responses and strong interferon-γ–producing and interleukin-2–producing CD8+ cytotoxic T-cell responses. This ability to elicit both humoral and cell-mediated antiviral mechanisms makes BNT162b1 a promising vaccine candidate.
Here, we report the full set of safety and immunogenicity data from the phase 1 portion of an ongoing randomized, placebo-controlled, observer-blinded, dose-escalation trial in the United States that was used to select the final vaccine candidate, as well as the comparison of the safety and immunogenicity of both vaccine candidates and additional phase 1 data that have been collected since candidate selection. These data include evaluation of the 10-μg, 20-μg, and 30-μg dose levels of BNT162b1 and BNT162b2 in adults 18 to 55 years of age and adults 65 to 85 years of age.
Methods
Trial Objectives, Participants, and Oversight
We assessed the safety and immunogenicity of three dose levels of BNT162b1 and BNT162b2. Healthy adults 18 to 55 years of age or 65 to 85 years of age were eligible for inclusion. Key exclusion criteria were known infection with human immunodeficiency virus, hepatitis C virus, or hepatitis B virus; an immunocompromised condition; a history of autoimmune disease; a previous clinical or microbiologic diagnosis of Covid-19; the receipt of medications intended to prevent Covid-19; any previous coronavirus vaccination; positive test for SARS-CoV-2 IgM or IgG at the screening visit; and positive nasal-swab results on a SARS-CoV-2 nucleic acid amplification test within 24 hours before the receipt of trial vaccine or placebo.
BioNTech was the regulatory sponsor of the trial. Pfizer was responsible for the trial design; for the collection, analysis, and interpretation of the data; and for the writing of the report. The corresponding author had full access to all the data in the trial and had final responsibility for the decision to submit the manuscript for publication. All the trial data were available to all the authors.
Trial Procedures
Using an interactive Web-based response technology system, we randomly assigned trial participants to groups defined according to the vaccine candidate, dose level, and age range. Groups of participants 18 to 55 years of age and 65 to 85 years of age were to receive doses of 10 μg, 20 μg, or 30 μg of BNT162b1 or BNT162b2 (or placebo) on a two-dose schedule; one group of participants 18 to 55 years of age was assigned to receive 100-μg doses of BNT162b1 or placebo. All the participants were assigned to receive two 0.5-ml injections of active vaccine (BNT162b1 or BNT162b2) or placebo into the deltoid, administered 21 days apart.
The first five participants in each new dose level or age group (with a randomization ratio of 4:1 for active vaccine:placebo) were observed for 4 hours after the injection to identify immediate adverse events. All the other participants were observed for 30 minutes. Blood samples were obtained for safety and immunogenicity assessments.
Safety
The primary end points in phase 1 of this trial were solicited local reactions (i.e., specific local reactions as prompted by and recorded in an electronic diary), systemic events, and use of antipyretic or pain medication within 7 days after the receipt of vaccine or placebo, as prompted by and recorded in an electronic diary; unsolicited adverse events and serious adverse events (i.e., those reported by the participants, without electronic-diary prompts), assessed from the receipt of the first dose through 1 month and 6 months, respectively, after the receipt of the second dose; clinical laboratory abnormalities, assessed 1 day and 7 days after the receipt of vaccine or placebo; and grading shifts in laboratory assessments between baseline and 1 day and 7 days after the first dose and between 2 days and 7 days after the second dose. Protocol-specified safety stopping rules were in effect for all the participants in the phase 1 portion of the trial. The full protocol, including the statistical analysis plan, is available with the full text of this article at NEJM.org. An internal review committee and an external data and safety monitoring committee reviewed all safety data.
Immunogenicity
Immunogenicity assessments (SARS-CoV-2 serum neutralization assay and receptor-binding domain [RBD]–binding or S1-binding IgG direct Luminex immunoassays) were conducted before the administration of vaccine or placebo, at 7 days and 21 days after the first dose, and at 7 days (i.e., day 28) and 14 days (i.e., day 35) after the second dose. The neutralization assay, which also generated previously described virus-neutralization data from trials of the BNT162 candidates,2,5 used a previously described strain of SARS-CoV-2 (USA_WA1/2020) that had been generated by reverse genetics and engineered by the insertion of an mNeonGreen gene into open reading frame 7 of the viral genome.11,12 The 50% neutralization titers and 90% neutralization titers were reported as the interpolated reciprocal of the dilutions yielding 50% and 90% reductions, respectively, in fluorescent viral foci. Any serologic values below the lower limit of quantitation were set to 0.5 times the lower limit of quantitation. Available serologic results were included in the analysis.
Immunogenicity data from a human convalescent serum panel were included as a benchmark. A total of 38 serum samples were obtained from donors 18 to 83 years of age (median age, 42.5 years) who had recovered from SARS-CoV-2 infection or Covid-19; samples were obtained at least 14 days after a polymerase chain reaction–confirmed diagnosis and after symptom resolution. Neutralizing geometric mean titers (GMTs) in subgroups of the donors were as follows: 90, among 35 donors with symptomatic infections; 156, among 3 donors with asymptomatic infection; and 618, in 1 donor who was hospitalized. Each serum sample in the panel was from a different donor. Thus, most of the serum samples were obtained from persons with moderate Covid-19 who had not been hospitalized. The serum samples were obtained from Sanguine Biosciences, the MT Group, and Pfizer Occupational Health and Wellness.
Statistical Analysis
We report descriptive results of safety and immunogenicity analyses, and the sample size was not based on statistical hypothesis testing. Results of the safety analyses are presented as counts, percentages, and associated Clopper–Pearson 95% confidence intervals for local reactions, systemic events, and any adverse events after the administration of vaccine or placebo, according to terms in the Medical Dictionary for Regulatory Activities, version 23.0, for each vaccine group. Summary statistics are provided for abnormal laboratory values and grading shifts. Given the small number of participants in each group, the trial was not powered for formal statistical comparisons between dose levels or between age groups.
Immunogenicity analyses of SARS-CoV-2 serum neutralizing titers, S1-binding IgG and RBD-binding IgG concentrations, GMTs, and geometric mean concentrations (GMCs) were computed along with associated 95% confidence intervals. The GMTs and GMCs were calculated as the mean of the assay results after the logarithmic transformation was made; we then exponentiated the mean to express results on the original scale. Two-sided 95% confidence intervals were obtained by performing logarithmic transformations of titers or concentrations, calculating the 95% confidence interval with reference to Student’s t-distribution, and then exponentiating the limits of the confidence intervals.
Results
Demographic Characteristics of the Participants
Screening and Randomization of the Participants.
Between May 4, 2020, and June 22, 2020, a total of 332 healthy adults (men and nonpregnant women) underwent screening at four sites in the United States (two sites per vaccine candidate). A total of 195 participants were randomly assigned to 13 groups comprising 15 participants each; in each group, 12 participants received vaccine and 3 received placebo (Figure 1). In all groups but one, all the participants who underwent randomization received the assigned two doses of vaccine or placebo. Participants 18 to 55 years of age who had been assigned to receive 100 μg of BNT162b1 or placebo received one dose; the second dose was not administered because of reactogenicity in the participants who received active vaccine.5
Demographic Characteristics of the Participants, According to Vaccine Candidate and Age Group.
The majority of participants were White (67 to 100%) and non-Hispanic (89 to 100%) (Table 1). More older women than older men participated. The median age among the younger participants was 35 years in the BNT162b1 group and 37 years in the BNT162b2 group; the median age among the older participants was 69 years and 68 years, respectively.
Safety
Local Reactions
Local Reactions Reported within 7 Days after the Administration of Vaccine or Placebo, According to Age Group.
Participants 18 to 55 years of age who received 10 μg, 20 μg, or 30 μg of BNT162b1 reported mild-to-moderate local reactions, primarily pain at the injection site, within 7 days after an injection; the local reactions were more frequent after the second dose.2,5 BNT162b1 elicited local reactions in similar proportions of the participants in the younger age group and in the older age group. Among the older participants, mild-to-moderate injection-site pain was reported by 92% after the first dose and by 75% after the second dose (Figure 2). A similar pattern was observed after vaccination with BNT162b2. No older participant who received BNT162b2 reported redness or swelling. No participant who received either BNT162 vaccine candidate reported a grade 4 local reaction.
Systemic Events
Selected Systemic Events Reported within 7 Days after the Administration of Vaccine or Placebo, According to Age Group.
Participants 18 to 55 years of age who received 10 μg, 20 μg, or 30 μg of BNT162b1 frequently had mild-to-moderate fever and chills, with 75% of the participants reporting a temperature of 38.0°C or higher after the second 30-μg dose (Figure 3; and Fig. S1 in the Supplementary Appendix, available at NEJM.org).5 In participants 65 to 85 years of age who received BNT162b1, systemic events were milder than in the younger participants, although many older participants reported fatigue and headache after the first or second dose, and 33% reported a temperature of 38°C or higher after the second dose, including one older participant who reported a fever of 38.9 to 40.0°C (Figure 3 and Fig. S2). As was observed with local reactions, systemic events were dose-dependent (greater after the second dose than after the first dose) and transient. Symptoms generally peaked by day 2 after vaccination and resolved by day 7.
Systemic events in response to BNT162b2 were milder than those in response to BNT162b1 (Figure 3 and Figs. S1 and S2). For example, 17% of the participants 18 to 55 years of age and 8% of those 65 to 85 years of age reported fever (≥38.0 to 38.9°C) after the second dose of 30 μg of BNT162b2. Severe systemic events (fatigue, headache, chills, muscle pain, and joint pain) were reported in small numbers of younger recipients of BNT162b2, but no severe systemic events were reported by older recipients of this vaccine candidate. No participant who received either BNT162 vaccine candidate reported a grade 4 systemic event. After the first dose, systemic events that were reported by participants 65 to 85 years of age who received BNT162b2 were similar to those reported by participants who received placebo.
In both age groups and for both vaccine candidates, the use of antipyretic or pain medication increased with increasing dose level and with the number of doses administered. Fewer BNT162b2 recipients than BNT162b1 recipients reported using antipyretic or pain medication.
Adverse Events and Shifts in Laboratory Values
Through 1 month after the receipt of the second dose, adverse events that were considered by the investigators to be related to vaccine or placebo were reported by 50% of the participants 18 to 55 years of age who received 30 μg of BNT162b1, as compared with 8% of those who received placebo.5 Adverse events that were considered to be related to vaccine were reported by 17% of the participants 65 to 85 years of age who received 30 μg of BNT162b1 and by 25% of the participants 18 to 55 years of age who received 30 μg of BNT162b2. No participant 65 to 85 years of age who received 30 μg of BNT162b2 reported a related adverse event (Table S1).
No serious adverse events were reported, and no stopping rules were met as of the time of this report. The largest changes from baseline in laboratory values were transient decreases in lymphocyte counts, which resolved within 1 week after vaccination (Fig. S3) and which were not associated with clinical manifestations.
Immunogenicity
Immunogenicity of BNT162b1 and BNT162b2.
The serologic responses elicited by BNT162b1 and BNT162b2 were similar (Figure 4). Two serum samples, both from the group of participants 18 to 55 years of age who received 30 μg of BNT162b2, were obtained outside the specified time windows (one each at day 28 and day 35) and thus were excluded from the reported immunogenicity analysis. Antigen-binding IgG and virus-neutralizing responses to vaccination with 10 μg to 30 μg of BNT162b1 or BNT162b2 were boosted by the second dose in both the younger adults2,5 and the older adults. Both vaccines elicited generally lower antigen-binding IgG and virus-neutralizing responses in participants 65 to 85 years of age than in those 18 to 55 years of age. Higher doses appeared to elicit somewhat higher antibody responses.
The highest neutralization titers were measured in samples obtained on day 28 (i.e., 7 days after the second dose) or on day 35 (i.e., 14 days after the second dose). Similar trends were observed for the 50% and 90% neutralizing titers (Fig. S4). The 50% neutralizing GMTs for the two vaccine candidates at the 30-μg dose level on day 28 or day 35 ranged from 1.7 to 4.6 times the GMT of the convalescent serum panel among participants 18 to 55 years of age and from 1.1 to 2.2 times the GMT of the convalescent serum panel among those 65 to 85 years of age. With 10 to 12 valid results per assay from samples that could be evaluated for each group at each time point, pair-wise comparisons are subject to error and have no clear interpretation.
Discussion
Previously reported data from vaccination with 10 μg or 30 μg of BNT162b1 in adults 18 to 55 years of age suggested that it could be a promising Covid-19 vaccine candidate.2,5 Consistent with our strategy to evaluate several RNA vaccine candidates and make a data-driven decision to advance the candidate with the best safety and immunogenicity profile, we compared clinical data obtained after vaccination with BNT162b1,2,5 which encodes the RBD, with data obtained after vaccination with BNT162b2, which encodes the full-length spike. The data presented here include those that guided our decision to advance BNT162b2 at the 30-μg dose level to the phase 2–3, international trial to evaluate its safety and efficacy in participants 18 to 85 years of age.
The primary consideration driving this decision was the milder systemic reactogenicity profile of BNT162b2, particularly in older adults, in the context of the similar antibody responses elicited by the two candidate vaccines. Short-lived decreases in postvaccination lymphocyte counts had no associated clinical effect, were observed across the age groups, and probably reflect a temporary redistribution of lymphocytes from the bloodstream to lymphoid tissues as a functional response to immune stimulation by the vaccine.13-16 The immune response and toxicity profile at the selected, relatively low, 30-μg dose level indicate that the BNT162b2 modRNA vaccine candidate has a favorable balance of reactogenicity and immunogenicity.17,18
The composition of the lipid nanoparticles, the formulation components, or the sequence selection for the vaccine RNA could influence the side-effect profile. The reason for the lower reactogenicity of BNT162b2 than of BNT162b1 is not certain, given that the two vaccine candidates share the same modRNA platform, RNA production and purification processes, and formulation of lipid nanoparticles. They differ in the nucleotide sequences that encode the vaccine antigens and in the overall size of the RNA constructs, which results in a number of RNA molecules in 30 μg of BNT162b1 that is approximately 5 times as high as that in 30 μg of BNT162b2. The nucleotide composition of RNA has been reported to affect its immune stimulatory activity and reactogenicity profile, and this is a possible explanation for the differences in these vaccine candidates.19
The immune responses elicited by BNT162b1 and BNT162b2 were similar. As has been observed with other vaccines and as is probably associated with immunosenescence,20,21 the immunogenicity of the two vaccine candidates decreased with age, eliciting lower overall humoral responses in adults 65 to 85 years of age than in those 18 to 55 years of age. Nevertheless, at 7 days and 14 days after the second dose, the 50% and 90% neutralizing GMTs that were elicited by 30 μg of BNT162b2 in older adults exceeded those of the convalescent serum panel. Antibody responses in both younger and older adults showed a clear benefit of a second dose.
This trial and interim report have several limitations. First, the relative importance of humoral and cellular immunity with regard to protection from Covid-19 has not yet been fully characterized. Although strong cell-mediated immune responses (Th1-biased CD4+ and CD8+) elicited by BNT162b1 have been observed and reported in the German trial,2 the cellular immune responses elicited by BNT162b2 are still being studied. Second, although the serum neutralizing responses that were elicited by the vaccine candidates relative to those elicited by natural infection are highly encouraging, the degree of protection against Covid-19 provided by this or any other benchmark is unknown. Third, the phase 1 portion of this trial tested many hypotheses and was not powered to make formal statistical comparisons. Fourth, the human convalescent serum panels that have been used by different vaccine developers are not standardized among laboratories, and each represents a unique distribution of donor characteristics and times of collection. Therefore, the serum panel that we used does not provide a well-controlled benchmark for comparisons of the serologic responses elicited by these two BNT162 vaccine candidates with those elicited by other Covid-19 vaccine candidates. Finally, the participants in this early-stage clinical trial were healthy and had limited racial and ethnic diversity as compared with the general population.
Many of the limitations cited above are being addressed in the international, phase 2–3 portion of this trial. In this later, pivotal part of the trial, we are assessing the safety and efficacy of two doses of 30 μg of BNT162b2 in up to 44,000 participants (randomly assigned in a 1:1 ratio to receive vaccine or placebo) from diverse backgrounds, including persons with stable chronic underlying health conditions, persons at increased risk owing to occupational exposure, and persons from racial and ethnic backgrounds at higher risk for severe Covid-19.22 We are conducting outreach to recruit trial participants from many backgrounds and are using U.S. Census data to locate trial sites in diverse communities.
Supported by BioNTech and Pfizer.
Disclosure forms provide by the authors are available with the full text of the article at NEJM.org.
Drs. Walsh and Frenck contributed equally to this article.
This article was published on October 14, 2020, at NEJM.org.
A data sharing statement provided by the authors is available with the full text of this article at NEJM.org.
We thank Carol Monahan and Deb Gantt (of Pfizer) for writing and editorial assistance with an earlier version of the manuscript; James Trammel (of Pfizer) for assistance with the statistical analysis in the generation of an earlier version of the manuscript; Tricia Newell, Nicole O’Regan, and Emily Stackpole (of ICON), for editorial assistance with an earlier version of the manuscript, which was funded by Pfizer; all the participants who volunteered for this trial; and the following persons for their contributions to this work: Angelica Kottkamp, Ramin Herati, Rebecca Pellet Madan, Mary Olson, Marie Samanovic-Golden, Elisabeth Cohen, Amber Cornelius, Laura Frye, Heekoung Youn, Baby Jane Fran, Kanika Ballani, Natalie Veling, Juanita Erb, Mahnoor Ali, Lisa Zhao, Stephanie Rettig, Hibah Khan, Harry Lambert, Kelly Hu, and Jonathan Hyde (all of New York University Langone Vaccine Center); Monica McArthur, Justin Ortiz, Rekha Rapaka, Linda Wadsworth, Ginny Cummings, Toni Robinson, Nancy Greenberg, Lisa Chrisley, Wanda Somrajit, Jennifer Marron, Constance Thomas, Kelly Brooks, Lisa Turek, Patricia Farley, Staci Eddington, Panagiota Komninou, Mardi Reymann, Kathy Strauss, Biraj Shrestha, Sudhaunshu Joshi, Robin Barnes, Roohali Sukhavasi, Myounghee Lee, Alyson Kwon, and Terry Sharp (all of the Center for Vaccine Development and Global Health, University of Maryland School of Medicine); Emily Pierce, Mary Criddle, Maryrose Laguio-Vila, Megan Helf, Madison Murphy, Maria Formica, and Sarah Korones (all of the University of Rochester and Rochester General Hospital); Amy Cline, Susan Parker, and Michelle Dickey (all of Cincinnati Children’s Hospital); Kristen Buschle (of Pfizer); Andrea Cawein, John L. Perez, Harpreet Seehra, Dina Tresnan, Robert Maroko, Helen Smith, Sarah Tweedy, Amy Jones, Greg Adams, Rabia Malick, Emily Worobetz, Erica Weaver, Liping Zhang, Carmel Devlin, Donna Boyce, Elisa Harkins Tull, Mark Boaz, Michael Cruz, and the staff of the Vaccines Clinical Assay Team and the Vaccines Assay Development Team (all of Cincinnati Children’s Hospital); and Corinna Rosenbaum, Christian Miculka, Andreas Kuhn, Ferdia Bates, Paul Strecker, and Alexandra Kemmer-Brück (all of BioNTech).
Author Affiliations
From the University of Rochester and Rochester General Hospital, Rochester (E.E.W., A.R.F.), Vaccine Research and Development, Pfizer, Pearl River (J.A., A.G., K.A.S., K.K., W.K., D.C., K.R.T., P.R.D., K.U.J., W.C.G.), and New York University Langone Vaccine Center and Grossman School of Medicine, New York (M.J.M., V.R.) — all in New York; Cincinnati Children’s Hospital, Cincinnati (R.W.F.); Vaccine Research and Development, Pfizer, Hurley, United Kingdom (N.K., S.L., R.B.); the University of Maryland School of Medicine, Center for Vaccine Development and Global Health, Baltimore (K.N., K.E.L.); Vaccine Research and Development, Pfizer, Collegeville, PA (P.L.); the University of Texas Medical Branch, Galveston (C.F.-G., P.-Y.S.); and BioNTech, Mainz, Germany (ÖT., U.Ş.).
Address reprint requests to Dr. Absalon at Pfizer, 401 N. Middletown Rd., Pearl River, NY 10965, or at judith.absalon@pfizer.com.
References (22)
1. Johns Hopkins University Coronavirus Resource Center. COVID-19 dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. 2020 (https://coronavirus.jhu.edu/map.html. opens in new tab).
2. Sahin U, Muik A, Derhovanessian E, et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T-cell responses. Nature 2020September30 (Epub ahead of print).
3. Pardi N, Tuyishime S, Muramatsu H, et al. Expression kinetics of nucleoside-modified mRNA delivered in lipid nanoparticles to mice by various routes. J Control Release 2015;217:345–351.
4. Karikó K, Muramatsu H, Welsh FA, et al. Incorporation of pseudouridine into mRNA yields superior nonimmunogenic vector with increased translational capacity and biological stability. Mol Ther 2008;16:1833–1840.
6. He Y, Zhou Y, Liu S, et al. Receptor-binding domain of SARS-CoV spike protein induces highly potent neutralizing antibodies: implication for developing subunit vaccine. Biochem Biophys Res Commun 2004;324:773–781.
7. Güthe S, Kapinos L, Möglich A, Meier S, Grzesiek S, Kiefhaber T. Very fast folding and association of a trimerization domain from bacteriophage T4 fibritin. J Mol Biol 2004;337:905–915.
10. Pallesen J, Wang N, Corbett KS, et al. Immunogenicity and structures of a rationally designed prefusion MERS-CoV spike antigen. Proc Natl Acad Sci U S A 2017;114(35):E7348–E7357.
14. Hopkins RJ, Daczkowski NF, Kaptur PE, et al. Randomized, double-blind, placebo-controlled, safety and immunogenicity study of 4 formulations of Anthrax Vaccine Adsorbed plus CPG 7909 (AV7909) in healthy adult volunteers. Vaccine 2013;31:3051–3058.
16. Lai L, Davey R, Beck A, et al. Emergency postexposure vaccination with vesicular stomatitis virus-vectored Ebola vaccine after needlestick. JAMA 2015;313:1249–1255.
17. Feldman RA, Fuhr R, Smolenov I, et al. mRNA vaccines against H10N8 and H7N9 influenza viruses of pandemic potential are immunogenic and well tolerated in healthy adults in phase 1 randomized clinical trials. Vaccine 2019;37:3326–3334.
20. Muñoz N, Manalastas R Jr, Pitisuttithum P, et al. Safety, immunogenicity, and efficacy of quadrivalent human papillomavirus (types 6, 11, 16, 18) recombinant vaccine in women aged 24-45 years: a randomised, double-blind trial. Lancet 2009;373:1949–1957.
Τον «κώδωνα του κινδύνου» έκρουσε για μια ακόμη φορά ο πρώην αντιπρόεδρος της Pfizer Δρ. Michael Yeadon, ο οποίος αναφέρθηκε στο «παιχνίδι» που παίζουν κυβερνήσεις και εταιρείες με τα εμβόλια του κορωνοϊού, αλλά κυριότερα στους κινδύνους που εγκυμονούν για τους εμβολιασμούς σε παιδιά. .
Όπως είπε ο δρ. Yeadon για ένα παιδί έχει 50- φορές μεγαλύτερο κίνδυνο να πεθάνει από ένα εμβόλιο για τον κορωνοϊό παρά από τον ιό τον ίδιο!
Ο πρώην αντιπρόεδρος της Pfizer έχει ταχθεί κατά των εμβολιασμών σε παιδιά, κάτι τόσο η Pfizer-BionTech όσο και η Moderna επιδιώκουν τους μαζικούς εμβολιασμούς παιδιών από 12 έως 15 (σε πρώτη φάση) παρά το γεγονός ότι τα παιδιά δεν κινδυνεύουν από τον COVID-19 όσο οι ενήλικες.
Η περίεργη αυτή εμμονή των μεγάλων φαρμακευτικών εταιρειών να εμβολιάσουν τον παιδικό πληθυσμό έχει προκαλέσει τον έντονο σκεπτικισμό από πολλούς επιστήμονες, μεταξύ αυτών και του δρ. Yeadon.
Ο πρώην αντιπρόεδρος της Pfizer έχει 30 χρόνια εμπειρίας στην ανάπτυξη εμβολίων για ιούς όπως ο Covid-19. Ο γιατρός όμως ανησυχεί για τα εμβόλια, καθώς όπως λέει είναι νέα και πειραματικά, καθώς δεν έχουν υποβληθεί στις απαραίτητες κλινικές δοκιμές, καθώς αυτές απαιτούν περίπου 2-3 χρόνια.
Επομένως, δεν έχουμε ακόμη επαρκή στοιχεία σχετικά με τις πιθανές βραχυπρόθεσμες ή μακροπρόθεσμες συνέπειες αυτών των εμβολίων και συνεπώς τα εκατομμύρια ατόμων που έχουν υποβληθεί σε εμβολιασμό συμμετέχουν σε ένα πείραμα.
pronews.gr και https://www.triklopodia.gr/%cf%80%cf%81%cf%8e%ce%b7%ce%bd-%ce%b1%ce%bd%cf%84%ce%b9%cf%80%cf%81%cf%8c%ce%b5%ce%b4%cf%81%ce%bf%cf%82-pfizer-%ce%b3%ce%b9%ce%b1-%ce%b5%ce%bc%ce%b2%ce%bf%ce%bb%ce%b9%ce%b1%cf%83%ce%bc%ce%bf%cf%8d/
Ποιος να το πίστευε ότι ο κινέζικος φασισμός θα απειλούσε τη χώρα της <<Ελευθερίας;>>
THIS WAS HIS ENTIRE QUOTE: A sobering reminder. It’s been almost sixty one years since Russia’s Khrushchev delivered this.
Do you remember September 29, 1959?
THIS WAS HIS ENTIRE QUOTE:Τα πιο κάτω ήσαν ατόφια και ξεκάθαρα τα λόγια του… “Your children’s children will live under communism, You Americans are so gullible. No, you won’t accept communism outright; but we will keep feeding you small doses of socialism until you will finally wake up and find you already have Communism. We will not have to fight you; We will so weaken your economy, until you will fall like overripe fruit into our hands.” “The democracy will cease to exist when you take away from those who are willing to work and give to those who would not.”
Nikita_S._Chruschtschow“
Do you remember what Russia’s Khrushchev said in 1959?
Remember, socialism leads to Communism. So, how do you create a Socialistic State?
There are 8 levels of control; read the following recipe:
1) Healthcare – Control healthcare and you control the people. Σ.γ.: Ελέγχεις ολόκληρο τον πληθυσμό μιας χώρας όταν τον υποβάλεις σε εγκεφαλόπλυση με τα ΜΜΕ πως θα πεθάνει από μια υποτιθέμενη πανδημία που σκοτώνει.
2) Poverty – Increase the poverty level as high as possible, poor people are easier to control and will not fight back if you are providing everything for them. Σ.γ.: Δώσε στους πειναλέους συσσίτια και τους κάνεις σκλάβους σου έτοιμους να πουλήσουν και την ψυχή τους στο διάολο αρκεί να επιβιώσουν και μια μέρα παραπάνω. Ο Klauss Swab τα έχει διευκρινήσει πλήρως στο βθιβλίο του Great Reset.
3) Debt – Increase the debt to an unsustainable level. That way you are able to increase taxes, and this will produce more poverty. Σ.γ.: Αύξηση των χρεών των πολιτών που αφελώς δανείζονταν από τις τράπεζες ώστε να ξεπουληθούν οι περιουσίες τους με ειδικούς νόμους υπέρ των τραπεζών όπως ο πτωχευτικός νόμος. Αποτέλεσμα τεράστιος αριθμός φτωχοαμερικάνων και φτωχοελλήνων θα ψάχνουν στους σκουπιδοτενεκέδες σαν τα ζόμπις που ζητούν σάρκες και τρώνε το ένα το άλλο.
4) Gun Control – Remove the ability to defend themselves from the Government That way you are able to create a police state. Σ.γ.: Μάζεψε τα όπλα για να μην γίνουν επικίνδυνα τα πεινασμένα, ξεδοντιάρικα σκυλιά.
5) Welfare – Take control of every aspect (food, housing, income) of their lives because that will make them fully dependent on the government. Σ.γ.: Εν ονόματι ενός ενιαίου ταμείου φτώχιας-δήθεν φιλανθρωπίας, θα ορίζεις τα πάντα, τη ζωή τους, την καλύβα που θα μένουν, και θα τους ελέγχεις απόλυτα με μια κάρτα επιδόματος ίσα-ίσα για να διατηρούνται τα κτήνη στη ζωή. Κινέζικος σοσιαλισμός λέγεται αυτό.
6) Education – Take control of what people read and listen to and take control of what children learn in school. Σ.γ.:Εκπαίδευση των παιδιών τους όπως οι εκπαιδευτές σκύλων. Θα μαθαίνουν ό,τι χρειάζονται για να συνεχίζουν να είναι δούλοι αδιαμαρτύρητα στην κτηνώδη ζωή τους.
7) Religion – Remove the belief in God from the Government and schools because the people need to believe in ONLY the government knowing what is best for the people. Σ.γ.: Η πίστη στον Θεό θα αντικατασταθεί από την πίστη και την αφοσίωση στον ΜΕΓΑΛΟ ΑΔΕΡΦΟ και το κράτος.
8) Class Warfare – Divide the people into the wealthy and the poor. Eliminate the middle class This will cause more discontent and it will be easier to tax the wealthy with the support of the poor. Σ.γ.: Διάλυση της μεσαίας τάξης που είναι οι πιο μορφωμένοι και οι περισσότερο επικίνδυνοι. Ο σκοπός είναι να απομείνουν δυο κατηγορίες ατόμων, οι ελάχιστοι πλούσιοι και οι πολλοί φτωχοί κι εξαθλιωμένοι. Οι κουρελιασμένοι και πάμφτωχοι αλήτες βλέποντας την ευμάρεια της μεσαίας τάξης θα αντιδράσουν και θα επαναστατήσουν άρα θα βοηθούν έμμεσα το κράτος να τους φορολογεί άγρια ώστε να εκλείψουν σαν μεσοαστοί.
A perfect parallel to the Democrat\LIBERAL agenda!!!!!
Sounds like Joe Biden’s agenda to me, so far, what do you think ????
HOPE YOU’LL PASS THIS ALONG
Ask your kids if they know who he is? His first name is Nikita.
Σ.γ.: Σίγουρα τα παιδιά σας δεν ξέρουν τίποτα από την Ιστορία γιατί ο σκοπός είναι να παραμένουν αγράμματοι ΔΟΥΛΟΙ-ΡΟΜΠΟΤ ανθρώπινα κτήνη.
O Γιώργος Ευαγγελάτος ψυχίατρος – ψυχαναλυτής παρέχει ψυχιατρική βοήθεια και συμβουλευτική σε ανθρώπους που αντιμετωπίζουν προσωπικές ή οικογενειακές ψυχολογικές και ψυχοκοινωνικές δυσκολίες. Μάθετε περισσότερα για εμάς εδώ.
 Ευαγγελάτος Γεώργιος")












Πρόσφατα Σχόλια